MedicoPlexus
Authors –
Dony Paul, Greshma Sunny, Irene Joshy, Liya Joseph
SYLLABUS
Part I
- History taking – plan of history taking, sections, questions.
- General state of health of the patient. Current state of health – study plan.
- Basic physical methods of examination the patient.
- Body constitution, constitutional types.
- Body temperature. Types of temperature curves.
- Some general skin changes.
- Examination of the head.
- Examination of the neck.
- Respiratory failure.
- Dyspnea. Changes in the frequency, type and rhythm of breathing.
- Cyanosis.
12 Cough. Sputum.
- Chest pain.
- Inspection of the chest, pathological chest deformities.
- Palpation of the chest- pathologic changes.
- Percussion of the lungs – principles, normal and pathological findings.
- Auscultation of the lungs – types of breathing and mechanism of formation of adventitious sounds .
- Spirometric test and blood gas analysis. Changes in lung diseases
- Thoracocentesis . Analysis of the pleural effusion.
- Arterial hypertension, blood pressure measurement.
- Clinical manifestations and types of left-sided heart failure.
- Clinical manifestations and types of right-sided heart failure.
- Premature beats, supraventricular tachycardias.
- Atrial fibrillation and flutter.
- Disturbances in the conducting system of the heart.
- Auscultation of the heart. Mechanisms of formation of heart sounds.
- Cardiac murmurs – characteristics of cardiac murmurs.
- Examination of the arteries and arterial pulse.
- Electrocardiography – normal pattern.
- Functional methods of examination of the cardiovascular system
- Acute renal failure.
- Nephrotic syndrome
- Nephritic syndrome
- Urine analysis- proteinuria, haematuria, pyuria, tests of urine dilution and concentration.
- Renal function examination.
- X-ray, isotopic and other imaging methods of examination of the urinary tract system
- Physical examination of the abdomen. Ascites.
- Signs and symptoms of the esophagus diseases, methods examination of the esophagus.
- Signs and symptoms of the stomach diseases, methods of examination of the stomach.
- Diarrhea. Constipation. Melena.
- Maldigestion and malabsorption syndromes.
- Signs and symptoms of the colon diseases. Methods of examination of the colon.
- Liver failure.
- Jaundice – types of jaundice, mechanisms.
- Portal hypertension – pathogenesis.
- Physical, functionl and imaging examination of the liver.
- Signs and symptoms of the pancreatic diseases. Physical and functional examination of the pancreas.
- Acute and chronic haemorrhage, anemia.
- Disease manifestations of bones and joints. Methods of examination.
Part II
- Acute tracheobronchitis, acute bronchitis, bronchiolitis.
- Chronic bronchitis – etiology, pathogenesis, clinical presentation, types, diagnosis.
- Bronchial asthma – etiology, pathogenesis, clinical presentation, types, diagnosis.
- Bronchiectasistic disease – etiology, pathogenesis, clinical presentation, diagnosis.
- Chronic obstructive pulmonary disease- etiology, pathogenesis, clinical presentation, diagnosis.
- Pulmonary embolism – etiology, pathogenesis, clinical presentation, diagnosis.
- Pneumonia – etiology, pathogenesis, classification.
- Lobar pneumonia – etiology, pathogenesis, pathomorphology, clinical picture, diagnosis.
- Bronchopneumonia – etiology, pathogenesis, clinical presentation, diagnosis.
- Non-bacterial pneumonia-viral, mycoplasma pneumoniae, chlamydia pneumoniae 61. Lung cancer – etiology, pathogenesis, clinical presentation, diagnosis.
- Abscess of the lung – etiology, pathogenesis, clinical presentation, diagnosis.
- Lung tuberculosis – etiology, pathogenesis, clinical presentation, diagnosis.
- Diseases of the pleura- pleurisy and hydrothorax
- Acute rheumatic fever- etiology, pathogenesis, pathomorphology, clinical presentation, forms diagnosis.
- Endocarditis – etiology, pathogenesis, clinical presentation, species diagnosis.
- Mitral insufficiency – etiology, pathomorphology, clinical presentation, diagnosis.
- Mitral stenosis – etiology, pathomorphology, clinical presentation, diagnosis.
- Aortic insufficiency – etiology, pathomorphology, clinical presentation, diagnosis.
- Aortic stenosis – etiology, pathophysiology, clinical presentation, diagnosis.
- Myocarditis.
- Pericarditis, pericardial adhesions – etiology, pathogenesis, clinical presentation, species diagnosis.
- Pulmonary heart disease – etiology, pathogenesis, clinical presentation and stage diagnosis.
- Arterial hypertension- etiology, pathogenesis, clinical presentation, stage diagnosis.
- Atherosclerosis – etiology, clinical presentation, diagnosis.
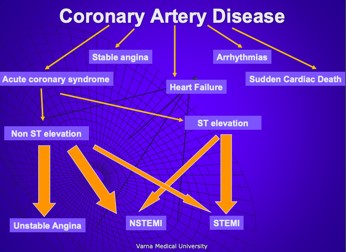
- Coronary artery disease – chronic coronary syndromes .
- Coronary artery disease – acute coronary syndromes- etiology, pathogenesis, clinical presentation, forms diagnosis.
- Coronary artery disease – acute coronary syndromes– clinical presentation, ECG changes, diagnosis.
- Acute diffuse glomerulonephritis – etiology, pathogenesis, pathomorphology, forms.
- Rapidly progressing (subacute) glomerulonephritis – etiology, pathogenesis, clinical presentation, diagnosis.
- Chronic glomerulonephritis – etiology, pathogenesis, morphology, forms, clinical presentation, diagnosis.
- Acute and chronic pyelonephritis – etiology, pathogenesis, morphology diagnosis.
- Nephrolithiasis – etiology, pathogenesis, clinical presentation, diagnosis.
- Kidney tumors – clinical presentation, diagnosis.
- Diseases of the esophagus (functional diseases, esophagitis, carcinoma) – etiology, pathogenesis, clinical presentation, diagnosis.
- Acute gastritis – etiology, pathogenesis, pathomorphology, clinical diagnosis.
- Chronic gastritis – etiology, pathogenesis, pathomorphology, forms, clinical presentation, diagnosis.
- Peptic ulcer – etiology, pathogenesis, clinical presentation, forms, complications, diagnosis.
- Gastric cancer. Etiology, pathogenesis, morphology, clinical presentation, forms diagnosis. 90. Acute and chronic colitis. Ulcerative colitis – etiology, pathogenesis, clinical presentation, diagnosis.
- Colon cancer – etiology, pathogenesis, clinical presentation, diagnosis.
- Chronic hepatitis – etiology, pathogenesis, clinical presentation, diagnosis.
- Liver cirrhosis – etiology, pathogenesis, classification, clinical picture, diagnosis.
- Liver cancer – etiology, pathogenesis, clinical presentation, diagnosis.
- Cholelithiasis and cholecystitis – etiology, pathogenesis, clinical presentation, diagnosis.
- Acute pancreatitis and chronic pancreatitis – etiology, pathogenesis, clinical presentation, diagnosis.
- Cancer of the pancreas – etiology, pathogenesis, clinical presentation, diagnosis.
- Chronic iron-deficiency anemia – etiology, pathogenesis, clinical presentation, diagnosis.
- Vitamin B12 and folic acid- deficiency anemia – etiology, pathogenesis, clinical presentation, diagnosis.
- Hemolytic anemia – etiology, pathogenesis, clinical presentation, diagnosis.
- Polycythemia – clinical presentation, diagnosis.
- Acute leukemia – etiology, pathogenesis, clinical, hematological forms, diagnosis. 103. Chronic myeloid leukemia – etiology, pathogenesis, clinical and hematologic presentation, diagnosis.
- Chronic lymphoid leukemia – etiology, pathogenesis, clinical and hematologic picture diagnosis.
- Agranulocytosis and pancytopenia – etiology, pathogenesis, clinical and hematologic presentation diagnosis.
- Bleeding disorders, types – etiology, pathogenesis.
- Hodgkin disease. Non-Hodgkin lymphomas- etiology, pathogenesis, clinical and hematologic picture diagnosis.
- Multiple myeloma- etiology, pathogenesis, clinical and hematological picture. 109. Acromegaly. Gigantism. Dwarfism – etiology, pathogenesis, clinical presentation, diagnosis.
10. Diabetes insipidus – etiology, pathogenesis, clinical presentation, diagnosis. 111. Thyrotoxicosis. Graves’ disease. Toxic adenoma-etiology, pathogenesis, clinical presentation, diagnosis.
- Hypothyroidism. Endemic and sporadic goiter. Cretinism – etiology, pathogenesis,
clinical presentation, diagnosis.
- Hyperparathyroidism – etiology, pathogenesis, clinical presentation, diagnosis.
- Hyperparathyroidism – etiology, pathogenesis, clinical presentation, diagnosis.
- Cushing disease and Cushing syndrome. Pheochromocytoma.
- Addison’s Disease and acute adrenal insufficiency – etiology, pathogenesis, clinical picture.
- Diabetes mellitus – etiology, pathogenesis, biochemistry.
- Diabetes mellitus – clinical picture, complications, diagnosis.
- Gout – etiology, pathogenesis, clinical presentation, diagnosis.
- Rheumatoid arthritis – etiology, pathogenesis, clinical presentation, diagnosis. 121. Ankylosing spondylitis (Bechterew disease) – etiology, pathogenesis, clinical presentation, diagnosis.
122. Osteoarthritis – etiology, pathogenesis, clinical presentation, diagnosis.
1. History taking – plan of history taking, sections, questions.
1-Generic: Name, age, DOB, Occupation, Gender, Address 2- Presenting/chief complaint 3- History of present complaint:
S-Site
O-onset (quick/slow)
C-character of pain
R-Radiation w
A-Associated factors (nausea/pain)
T-Timing
E-Exacerbating/ alleviating factors S-Severity 1-10
4- Past medical history:
- General: J-Jaundice. A-Anemia. D-Diabetes. E-Epilepsy
- Respiratory: T-TB. A-Asthma. B-Bronchitis
- Cardiovascular system: M-MI, A-Angina, R-Rheumatic fever. C-Cholesterol. HHypertension
5-Drug history/ Medications
Name, dose, frequency, route
6-Allergies
7-Family history
8-Social history: Smoking, drinking, drugs, ADL’s
Follow up by ICE = ideas, concerns, expectations of the patient
2. General state of health of the patient. Current state of health – study plan.
General Survey
- Apparent State of Health – acutely and chronically ill, frail, feeble, robust
- Levels of consciousness – awake, alert, responsive
- Signs of Distress and position in bed – dyspnea, pain, anxiety
- Height and Built
- Weight -emaciated, slender, obese
- Skin and mucous membranes – color and lesions
- Dress, grooming, and personal hygiene
- Facial expression
- Odors of body and breath
- Posture, gait and motor activity
Level of consciousness
- Levels of consciousness – awake, alert, responsive
- Levels of consciousness impairment
- Obnubilation – dizziness-awake, adequate, responsive, sluggish
- Somnolence-sleepiness – sleepy, slow, non adequate, responsive
- Sopor – not adequate, sleepy, partially responsive, tendon, corneal, pupil and gag reflexes
- Coma – unconscious, unresponsive only sluggish pupil reflexes
• Qualitative changes in consciousness
- Delirium – awake, hyperresponsive, not adequate, hyperactive, aggressive
- Amentia – awake, not adequate, responsive, disorientated, cognitive impairment
Comas
• Coma-total lack of consciousness, sensorium, conditional reflexes, voluntary motion, present depressed breathing, cardiac activity, blood pressure, pupil and gag reflexes • Types – intoxication, stroke, trauma, diabetes (ketoacidosis, hyperosmolar, lactic acidosis) hepatic and renal failure (hepatarghia, uremia)
Signs of distress and position in bed – dyspnea, pain, anxiety
- Active position – normal locomotion in bed, self service
- Passive position –no active locomotion, only passive mobility, in situations of impaired consciousness and grave deterioration of apparent state of health
- Compulsory position
- Sitting – in pulmonary edema and cardiac asthma in acute heart failure
- Lying – in acute abdomen in severe pain and distress
Height and Built
- Gigantism -Tall – over 190 cm in acromegaly, Kleinfelter syndrome, in Marfan syndrome
- Nanism – Small – under 100 cm, in various forms of dwarfism, in hypophyseal nanism (also hypopituitary nanism)
Weight — emaciated, slender, obese
- Normal – 20-24
- Overweight – 25-29
- Obesity >30
- Moderate >30
- Moderate >35
- Severe >40
Emaciated
- Inanition in anorexia nervosa, in stringe diets
- Cachexia in neoplastic disease
- Marasmus in semi and hyperdynamic states
Obesity
- Brocca-Weight = Height-100
- BMI-weight(kg)/height(m2)
- Basic physical methods of examining the patient.
The methods of physical examination are inspection, palpation, percussion, auscultation and mensuration.
The sequence of internal medical examination is:
- general survey
- head and neck
- chest and lung
- heart and cardiovascular system
- abdomen and gastrointestinal system joint examination
Methods of physical examination
1. Direct examination by the human senses and simple devices – ophthalmoscope, otoscope, flashlight/penlight, tongue depressors, ruler, thermometer,
sphygmomanometer, stethoscope, reflex hammer, tuning fork, safety pins, cotton for testing light touch
Inspection, palpation, percussion, auscultation, mensuration
- Position of the physician and patient, warm hands, tangential light
- Inspection – general, local, comparative, lighting, scopes – oto, rhino, ophthalmo, endo
- Palpation – superficial, deep –counter and sliding, local with rebound tenderness, combined, thrust, bimanual
- Percussion – pleximeter and plexor finger, percussion note-flat, dull, resonant, hyperresonant, tympanic – resonance (heard over lungs), tympany (heard over
the air-filled bowel loops), and dullness (heard over fluid or solid organs).Hyperresonant (pneumothorax)
- Auscultation – direct and indirect, selective
- Mensuration – body diameters, body constitution,BMI, BSA
- Succusio – kidney, liver -Costovertebral angle tenderness (CVAT), also known as
CVA tenderness, Murphy’s punch sign, Pasternacki’s sign, or Goldflam’s sign (Latin: succusio renalis), is a medical test in which pain is elicited by percussion of the area of the back overlying the kidney
● Murphy’s sign is elicited in patients with acute cholecystitis by asking the patient to take in and hold a deep breath while palpating the right subcostal area. If pain occurs on exspiration, when the inflamed gallbladder comes into contact with the examiner’s hand, Murphy’s sign is positive
4. Body constitution. Constitutional types
Constitution
The ratio of body parts-head, corpus and extremities
Diameter Of The Thorax-AP,sagittal and transverse
Ratios
Types
- Astenic-more often asthma and peptic
- Normosthenic
- Hypersthenic-more often diabetes, hypertension and myocardial infarction
| Sthenic | Asthenic | Hypersthenic | |
| Heart | Moderately transverse | Nearly vertical and
at midline | Axis nearly transverse |
| Lungs | Moderate length | Long, apices above clavicles, may be broader above base | Short, apices at or near clavicles |
| Diaphragm | Moderately high | Low | High |
| Stomach | High, upper left | Low and medial, in the pelvis when standing | High, transverse, and in the middle |
| Colon | Spread evenly; slight dip in transverse colon | Low, folds on itself | Around periphery of abdomen |
| Gallbladder | Centered on right
side, upper abdomen | Low and nearer the midline | High, outside, lies more parallel |
| Build | Moderately heavy | Frail | Massive |
| Abdomen | Moderately long | Short | Long |
| Thorax | Moderately short, broad, and deep | Long, shallow | Short, broad, deep |
| Pelvis | Relatively small | Wide | Narrow |
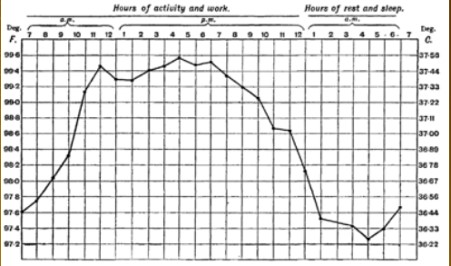
5. Body temperature. Types of temperature curves.
- Normal body temperature: 37C.
- Rectal, vaginal, otic is about 37.6C
- Oral is 36.8C+/- 0.7C
- Axillary is 36.6C
Diurnal (during the day) body temperature- circadian rhythm
 Physical signs of fever
Physical signs of fever
●Lethargy (lack of energy), depression,
anorexia, sleepiness, hyperalgesia
- Skin changes, febrile face
- Heart rate-tachycardia (proportional to temperature 10C=10 beats/min
- Chills/rigors
- Sweats/ night sweats
Temperature classification ● Normal 36.5-37.5C
- Hypothermia <35.0C
- Fever 37.5-38.3C
- Hyperthermia 38.4-39.9C
- Hyperpyrexia 40-41.5C
4 Stages of fever
- Prodromal: release of endogenous pyrogens, resetting of hypothalamus thermostatic set point to a higher level. Non specific complaints as fatigue as fatigue, headache, fleeting pain.
- Chill: Heat production prevails over heat emission, body temperature gradually rises, vasoconstriction, piloerection, shivering, skin is pale, goosebumps.
- Flush: Heat production becomes equal to heat emission= equilibrium. Patient feels heat flow, higher skin temperature.
- Defervescence: IL-1 decreases= diminishes heat production in muscles and liver, sweating, lowering in body temperature this can be rapid or quick.
Types of temperature curves
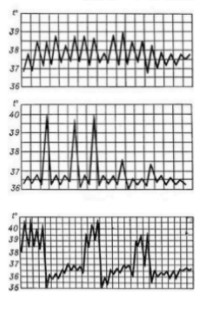 1. Febris continua: A constant fever the person maintains a temperature over 38C for at least a few days with fluctuations of 1C. Common in lobar pneumonia, purulent meningitis and typhus.
1. Febris continua: A constant fever the person maintains a temperature over 38C for at least a few days with fluctuations of 1C. Common in lobar pneumonia, purulent meningitis and typhus.
2.Febris remittens: relapsing fever, the temperature is above 39C, fluctuations of 1C never reaches the normal level. Common in viral and bacterial infections.
3.Febris intermittens: Intermittent fever temperature rises to 39/40C. Typical in malaria. Afebrile periods depend on the malaria plasmodium. Also found in mononucleosis and cytomegalovirus.
4. Febris recurrens: A recurrent fever of several days fever alternates with days of normal temperature. Common in typhus.
Fever of 24 hours;quotidian, 48 hours; tertian fever, 72 hours; quartan fever in plasmodium malariae.
Fever of unknown origin
- Infections
- Neoplasm
- Hematological
- Leukemia
- Local wounds/ DVT
Usefulness of fever
- Increased motility of leukocytes
- Enhanced leukocyte phagocytosis
- Endotoxin effects decreased
- Increased proliferation of T cells
- Enhanced activity of interferon
Management
- Fever does not always need to be treated
- At hyperpyrexia aggressive cooling is required
If temperature is elevated repeat readings hourly until stable.
6. Some general skin changes
Changes in skin and mucous membranes
Color
- Pale – anemia
- Cyanosis – reduced hemoglobin <50g/l
- central – respiratory failure
- peripheral – heart failure
- mixed – respiratory and heart failure
- Jaundice (icterus) = Yellow staining of skin and sclerae due to abnormally high blood levels of bile pigment bilirubin
- Melanodermia = Darkening of the skin due to an increased amount of melanin
- Vitiligo = Skin turns white due to lack of melanin
Primary skin lesions

- Macula = flat, non-palpable change in skin colour
- Telangiectasia = dilatation of capillaries causing them to appear as small red or purple clusters, often spidery in appearance
- Hemorrhagic = petechiae, purpura, ecchymosis, vibices, suffusions, sugilatio – vitropression
- Petechiae = small red or purple spot caused by bleeding into the skin due to capillary breaking
- Purpura = a rash of purple spots on the skin when small blood vessels burst, causing blood to pool under the skin
- Ecchymosis = Discoloration of the skin resulting from bleeding underneath, typically caused by bruising. Impact causes blood vessel to burst open leaking blood under the skin
- Vibices = Pale marks on a dead person’s skin caused by dermal pressure
- Suffusions = spreading of a fluid of the body into the surrounding tissues
- Sugilatio – vitropression = method of temporarily eliminating redness of the skin caused by hyperemia by pressure with a glass slide on the skin. Done with purpose of studying any lesions or discolorations
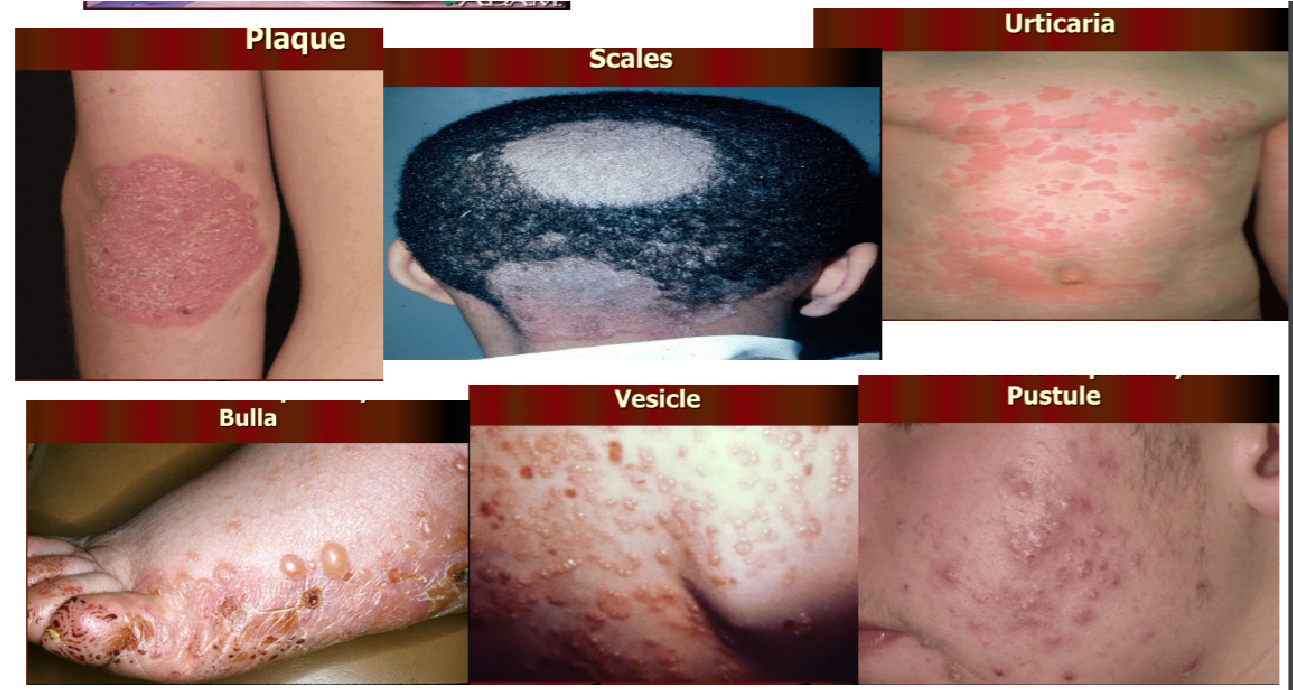
- Papule = a small pimple or swelling on the skin, often forming part of a rash
- Plaque = small, abnormal patch of tissue on a body part or an organ
- Scales = a visible peeling or flaking of outer skin layers. These layers are called the stratum corneum
- Urticaria = Another name for hives. Raised, itchy areas of skin that are usually a sign of an allergic reaction
- Bulla = A fluid-filled blister with thin walls. Bulla on the pleura is also called a bleb. One of the most common causes is friction. More than 5mm in diameter
- Vesicle = small blister on the skin. Also occur on the mucous membranes, such as the buccal mucosa. Less than 5mm in diameter.
10.Pustule = small collection of pus in the top layer of skin (epidermis) or beneath it in the dermis. Frequently form in sweat glands or hair follicles
Other skin lesions
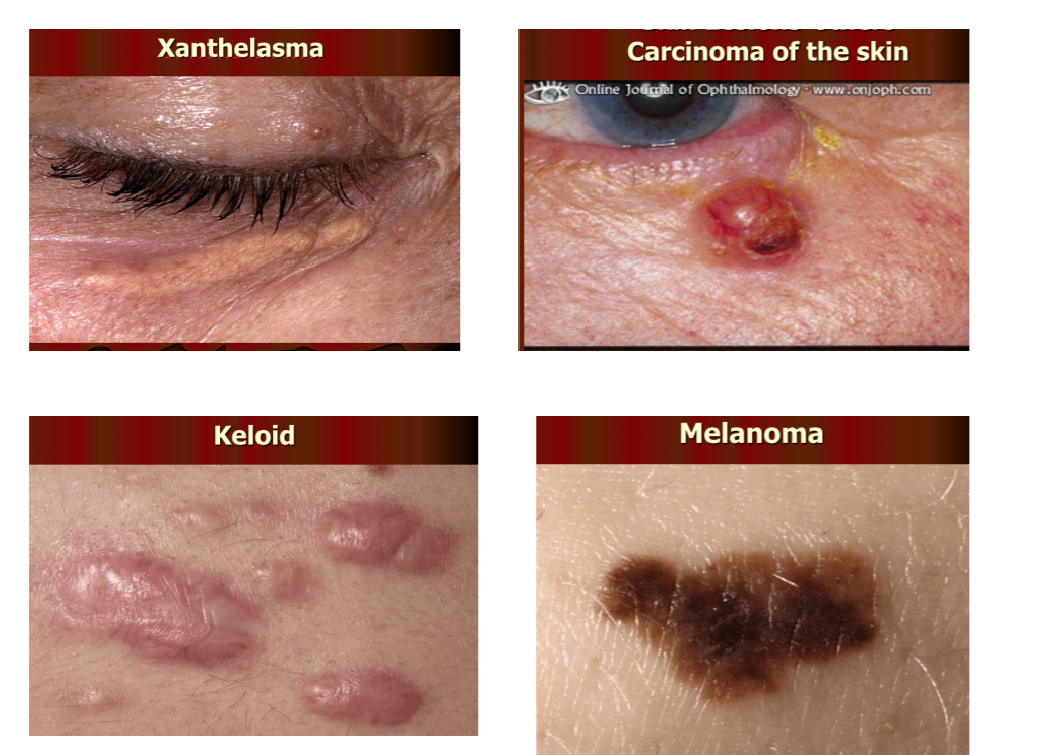

- Xanthelasma = yellowish deposit of cholesterol underneath the skin
- Carcinoma of skin = abnormal growth of skin cells
- Keloid = abnormal proliferation of scar tissue that forms at site of injury
- Melanoma = a cancer of the melanocyte
5. Crusta
- Nevi = A pigmented spot on the skin, such as a mole
- Erosion = loss of part or all of the epidermis
- Nails – onychomycosis, pigmentation, clubbing, arachnodactyly
- Onychomycosis – fungal infection of the nail
- Pigmentation – colouring
- Clubbing – bulbous enlargement of the ends of fingers or toes
- Arachnodactyly – abnormally long and slender fingers and toes
7. Examination of the head.
Overall Inspection
- Looking at the head and neck: paleness or yellow coloring of the sclera, the facial skin
- What do the lips look like? Cyanosis, Blisters (e.g herpes simplex)
- Facial features (Hypomimia)
- Stasis signs of neck veins
- Hematoma
Examination of the oral cavity
Opening the mouth with wooden spatula:
- Tooth status: carious, healthy, unobstructive)
- Gums: discoloration, bleeding
- Tongue: size, shape, aphthae (ulcus), congestion of the tongue veins
-
- Assessing the lingual frenulum (shortened?)
- Moisture tongue/mucous membranes: whitish pads (leukoplakia)
-
- Tonsils: mucus and pus on the tonsils
- Ductus parotideus: Visible, enlarged
Examination of the eyes Inspection:
- Width and shape of the pupils, symmetry (Anisocoria, Miosis or Mydriasis)
- Color (e.g. jaundice, redness) and humidity of the sclera
(e.g. Sicca symptoms)
- Iris color (e.g. Kayser-Fleischer-Kornealring)
- Light reaction: direct and indirect light
➔ Eye movement test: patient follows the movement of the index-finger only the eyes move without the
movement of the head
- Direction of movement
-
- Cranial 4 (Trochlear): innervates the superior oblique
- Cranial Nerve 6 (Abducens): innervates the lateral rectus
- Cranial Nerve 3 (Oculomotor): innervates all the remaining muscles (ie medial rectus, inferior oblique, superior rectus and inferior rectus)
-
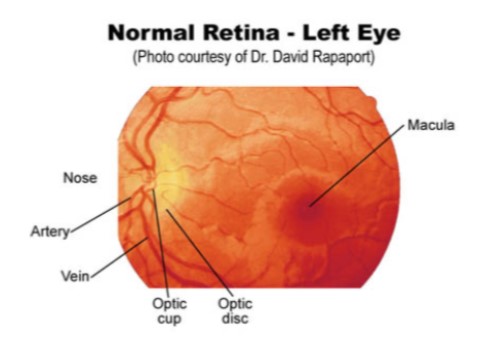
- Viewing fundus (retina and associated structures
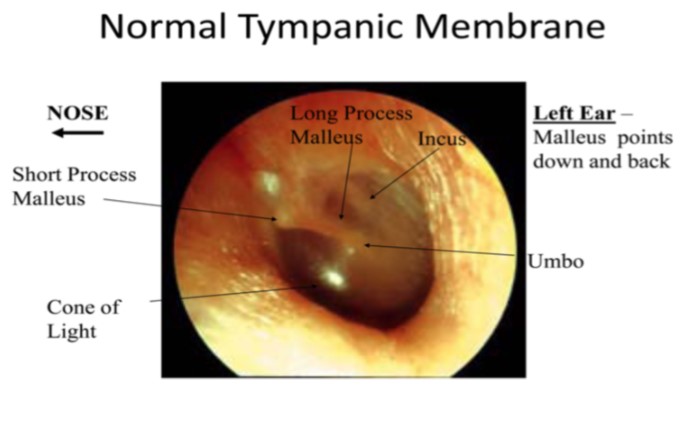 Examination of the ears
Examination of the ears
- look for swelling due to infection in external ear
- method: otoscope (speculum and viewing window)
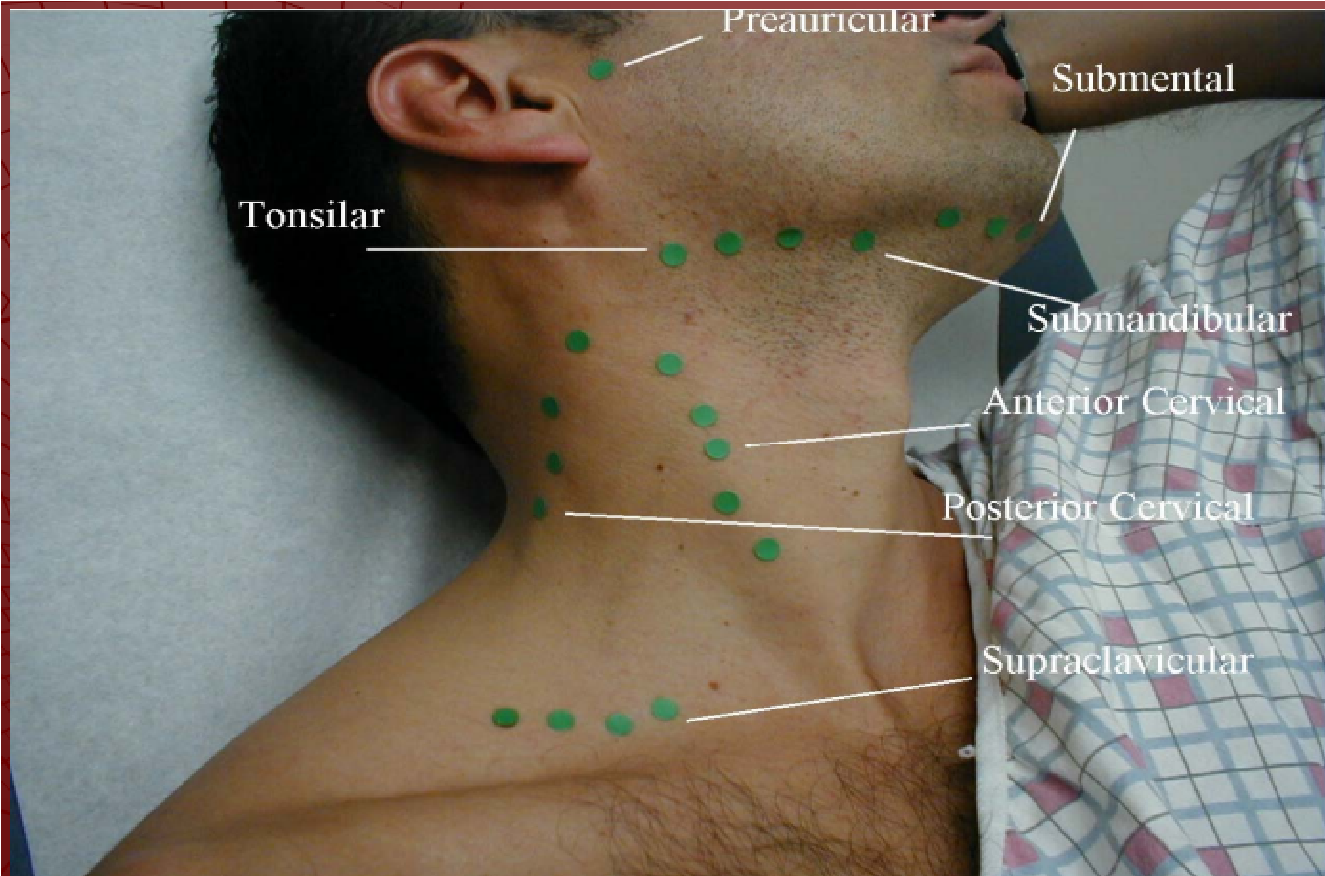
8. Examination of the neck https://geekymedics.com/neck-lumpexamination-osce-guide/
NECK EXAMINATION OUTLINE
- Review Pertinent Anatomy
- Landmarks
- Lymph Nodes
- Inspection
 Symmetry
Symmetry- Masses, Enlargements
- Scars
- Lymph Node Palpation
- Preauricular
- Posterior Auricular
- Occipital
- Tonsillar
- Submaxillary
- Submental
- Superficial Cervical
- Deep Cervical Chain
- Posterior Cervical Chain
- Supraclavicular
- THYROID GLAND EXAMINATION
- Technique
- Abnormalities
- Single nodule
- Multiple nodules
- Diffuse goiter
Thyroid inspection
View from the front: —> ask for slight reclination of the head —> look for bulge/asymmetry —> Abnormalities: single nodule, multiple nodule, diffuse goiter
Investigation: – Approach patient for the examination from behind and put your hands loosely on his neck – Fingers (are caudal and sideways) and slip between the larynx and M.
Sternocleidomastoideus
Palpation: Thyroid palpate: consistency, pain, knot
Swallow movement of patient: movement of thyroid palpable
9. Respiratory failure
Respiratory failure is a condition in which your blood doesn’t have enough oxygen or too much carbon dioxide. Sometimes both. Failure in efficient gas exchange. This results in not enough oxygen reaching vital organs.
Chronic respiratory failure-extra pulmonary and pulmonary ventilation/perfusion mismatch, diffusion changes. Grade 1 hypoxemia- SOB & cyanosis
Grade 2 hypoxemia and hypercapnia- SOB, cyanosis and bounding pulses Grade 3 hypoxemia, hypercapnia and respiratory acidosis-SOB, cyanosis, bounding pulses and mental changes
Acute respiratory failure occurs when fluid builds up in the air sacs in your lungs. Lungs can no longer release oxygen into your blood. Acute respiratory failure is a medical emergency.
Causes
- Lung diseases such as COPD, CF, pneumonia and pulmonary embolism
- Amyotrophic lateral sclerosis (ALS), muscular dystrophy, spinal cord injuries, stroke or any other condition which affects the nerves and muscles which control breathing.
- Scoliosis
- Damage to tissues and ribs around the lungs, trauma.
- Drugs or alcohol overdose
- Inhalation injuries (eg. smoke intake)
Chest X-ray, EKG- arrhythmias are common.
Treatment
- Oxygen therapy
- Tracheostomy
- Ventilator
- Fluids
- Treating the cause
10. Dyspnea. Changes in the frequency, type and rhythm of breathing.
Dyspnea
Shortness of breath. It can be acute (sudden dyspnea) or chronic (long-lasting dyspnea). Acute dyspnea starts within a few minutes or hours. It can happen with other symptoms like a fever, rash, or cough. Chronic dyspnea can make you feel out of breath with everyday tasks, such as walking from room to room or standing up
Symptoms:
- Out of breath
- Tightness in chest
- Hungry for air (air hunger)
- Unable to breathe deeply
- Can’t breathe (suffocation)
Most common causes:
- Asthma
- Heart failure
- Chronic obstructive pulmonary disease
- Interstitial lung disease
- Pneumonia
- Psychogenic problems that are usually linked to anxiety
Respiration
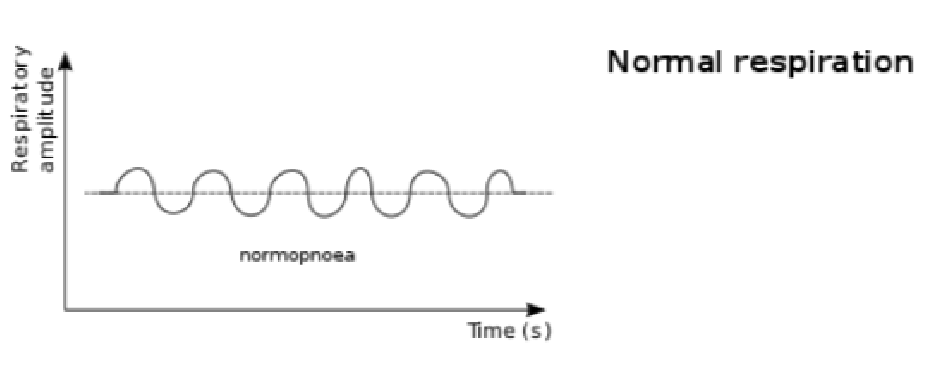 Rate = adult – 14-20 cycles/minute; newborn – 44 cycles/minute
Rate = adult – 14-20 cycles/minute; newborn – 44 cycles/minute- Should be counted for one minute
- Tachypnea-dyspnea, fever
- Bradypnea- uremia, drugs, narcotics, etc
Types of breathing and mechanism of formation – (changes)
• Hyperpnea – increased depth and rate of breathing. May be physiologic, as when required to meet metabolic demand of body tissues (for example, during or after exercise, or when the body lacks oxygen at high altitude or as a result of anemia). It may be pathologic, as when sepsis is severe
Kussmaul breathing
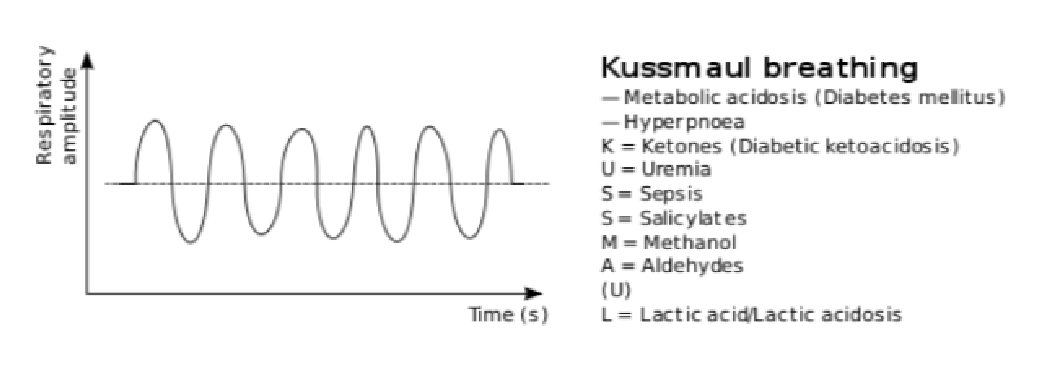 rate/variable
rate/variable- deep laboured breathing pattern
- is a form of hyperventilation (more respirations to decrease CO2)
- associations: diabetic ketoacidosis (DKA), uremia, metabolic acidosis, pneumonia
Cheyne- Stokes
- abnormal pattern of breathing
- Progressively deeper, and sometimes faster breathing followed by a gradual decrease that results in a temporary stop in breathing (apnea) • Pattern repeats, each cycle = 30 seconds to 2 minutes long
- Association / clinical occurrence:
- normal
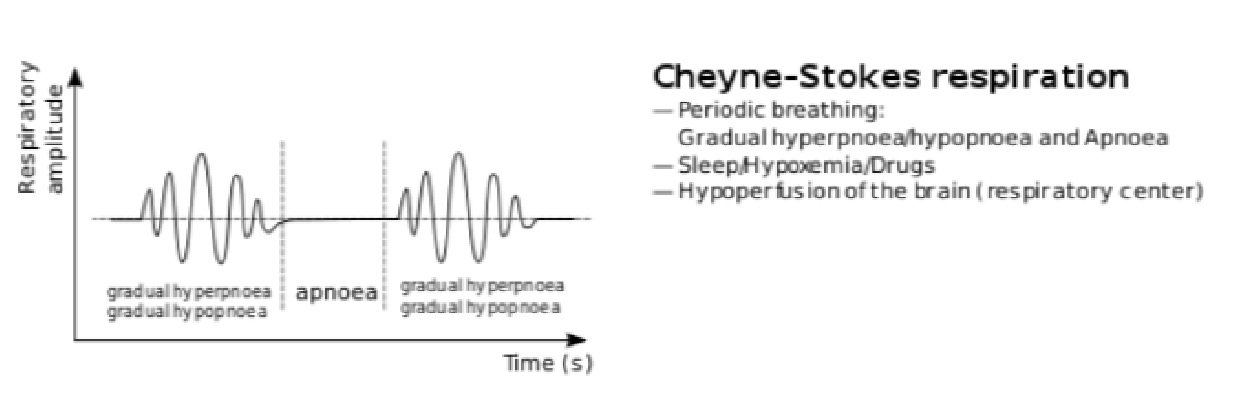 during sleep in children and aged
during sleep in children and aged- various pathologies
- heart failure
- brain damage
- increased intracerebral pressure secondary to numerous causes
- drug induced respiratory depression
Biot’s respirations
• abnormal pattern of breathing characterised by groups of quick, shallow inspirations followed by regular or irregular periods of apnea • associations/ clinical occurrence:
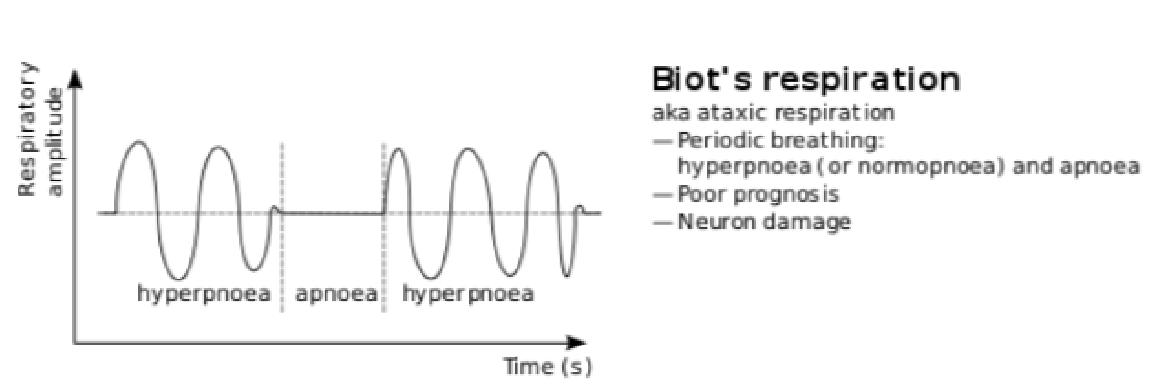 – damage to the pons due to strokes or trauma or by pressure on the pons
– damage to the pons due to strokes or trauma or by pressure on the pons
due to uncal or tentorial herniation – can be caused by opioid use
11. Cyanosis
= Bluish discoloration of the skin and/or mucous membranes are usually due to elevated quantity of reduced hemoglobin (>40 g/L [>4 g/dL]) in the capillary blood vessels.
Findings are most apparent in the lips, nail beds, ears, and malar eminences.
Central cyanosis:
- Results from arterial desaturation or presence of an abnormal hemoglobin.
- !”#$%%&’()*+(,-’./(,’$0-(0*$%’”$-#0$-*1,’*”’23456’10’
 2745’*,’+$089″8*,,(+’*,+*)*+#$%”:’
2745’*,’+$089″8*,,(+’*,+*)*+#$%”:’
Etiologies include:
- Impaired pulmonary function: Poorly ventilated alveoli or impaired oxygen diffusion; most frequent in pneumonia, pulmonary edema, and chronic obstructive pulmonary disease (COPD); in COPD with cyanosis, secondary polycythemia is often present.
- Anatomic vascular shunting: Shunting of desaturated venous blood into the arterial circulation may result from congenital heart disease or pulmonary atrioventricular (AV) fistula.
- Decreased inspired O2: Cyanosis may develop in ascents to altitudes >4000 m (>13,000 ft).
- Abnormal hemoglobins: Methemoglobinemia,
sulfhemoglobinemia, and mutant hemoglobins with low oxygen affinity (see Chap. 127, HPIM-19).
Peripheral cyanosis:
- Occurs with normal arterial O2 saturation with increased extraction of O2 from capillary blood caused by decreased localized blood flow.
 Contributors include vasoconstriction due to cold exposure, decreased cardiac output (e.g., in shock), heart failure , and peripheral vascular disease with arterial obstruction or vasospasm.
Contributors include vasoconstriction due to cold exposure, decreased cardiac output (e.g., in shock), heart failure , and peripheral vascular disease with arterial obstruction or vasospasm.- Local (e.g., thrombophlebitis) or central (e.g., constrictive pericarditis) venous hypertension intensifies cyanosis.
APPROACH TO THE PATIENT: Cyanosis
- Inquire about duration (cyanosis since birth suggests congenital heart disease) and exposures (drugs or chemicals that result in abnormal hemoglobins).
- Differentiate central from peripheral cyanosis by examining nail beds, lips, and mucous membranes. Peripheral cyanosis is most intense in nail beds and may resolve with gentle warming of extremities.
- Check for clubbing, i.e., selective enlargement of the distal segments of fingers and toes, due to proliferation of connective tissue. Clubbing may be hereditary, idiopathic, or acquired in association with lung cancer, infective endocarditis, bronchiectasis, or hepatic cirrhosis. Combination of clubbing and cyanosis is frequent in congenital heart disease and occasionally in pulmonary disease (lung abscess, pulmonary AV shunts, but not with uncomplicated obstructive lung disease).
- Examine chest for evidence of pulmonary disease, pulmonary edema, or murmurs associated with congenital heart disease.
- If cyanosis is localized to an extremity, evaluate for peripheral vascular obstruction.
- Obtain arterial blood gas to measure systemic O2 saturation. Repeat while pt inhales 100% O2; if saturation fails to increase to >95%, intravascular shunting of blood bypassing the lungs is likely (e.g., right-to-left intracardiac shunts).
- Evaluate for abnormal hemoglobins (e.g., spectroscopy, measurement of methemoglobin level).
12. Cough. Sputum
Coughing is your body’s way of getting rid of an irritant. When something irritates your throat or airway, your nervous system sends an alert to your brain. Your brain responds by telling the muscles in your chest and abdomen to contract and expel a burst of air.A cough is an important defensive reflex that helps protect your body from irritants like Mucus, Smoke and allergens, such as dust, mold, and pollen. Coughing is a symptom of many illnesses and conditions. Sometimes, the characteristics of your cough can give you a clue to its cause. Coughs can be described by:
- Behavior or experience. When and why does the cough happen? Is it at night, after eating, or while exercising?
- Characteristics. How does your cough sound or feel? Hacking, wet, or dry?
- Duration. Does your cough last less than 2 weeks, 6 weeks, or more than 8 weeks?
- Effects. Does your cough cause related symptoms such as urinary incontinence, vomiting, or sleeplessness?
- Grade. How bad is it? Is it annoying, persistent, or debilitating?
There are many different types of cough:
- Wet cough
- Dry cough
- Paroxysmal cough
- Croup cough
Wet cough
A wet cough, also called a productive cough, is a cough that typically brings up mucus.A cold or the flu commonly causes wet coughs. They can come on slowly or quickly and may be accompanied by other symptoms, such as runny nose, postnasal drip and fatigue.Wet coughs sound wet because your body is pushing mucus out of your respiratory system, which includes your throat, nose, airways and lungs. If you have a wet cough, you may feel like there’s something stuck or dripping at the back of your throat or in your chest. Some of your coughs will bring mucus into your mouth. Wet coughs can be acute and last less than 3 weeks or chronic and last longer than 8 weeks in adults or 4 weeks in children. Conditions that can cause a wet cough include:
| ● | a cold or the flu |
| ● | pneumonia |
| ● | chronic obstructive pulmonary disease (COPD), including emphysema and chronic bronchitis |
| ● | acute bronchitis |
| ● | Asthma |
Dry cough
A dry cough is a cough that doesn’t bring up mucus. It may feel like you have a tickle in the back of your throat triggering your cough reflex, giving you hacking coughs.Dry coughs are often difficult to manage and may present in long fits. Dry coughs occur because there’s inflammation or irritation in your respiratory tract, but there’s no excess mucus to cough up.Dry coughs are often caused by upper respiratory infections, such as a cold or the flu. In both children and adults, it’s common for dry coughs to linger for several weeks after a cold or the flu has passed. Other possible causes of dry cough include laryngitis, sore throat, croup, tonsillitis, sinusitis, asthma, allergies, gastroesophageal reflux disease (GERD), medications, especially ACE inhibitors and exposure to irritants such as air pollution, dust, or smoke.
Paroxysmal cough
A paroxysmal cough is a cough with intermittent attacks of violent, uncontrollable coughing. A paroxysmal cough feels exhausting and painful. People struggle to get a breath and may vomit.
Pertussis, also known as whooping cough, is a bacterial infection that causes violent coughing fits. Other possible causes of a bad coughing fit include asthma, COPD, pneumonia, tuberculosis and choking.
Croup cough
Croup refers to an infection of the upper airway, which obstructs breathing and causes a characteristic barking cough. The cough and other signs and symptoms of croup are the result of swelling around the voice box (larynx), windpipe (trachea) and bronchial tubes (bronchi)
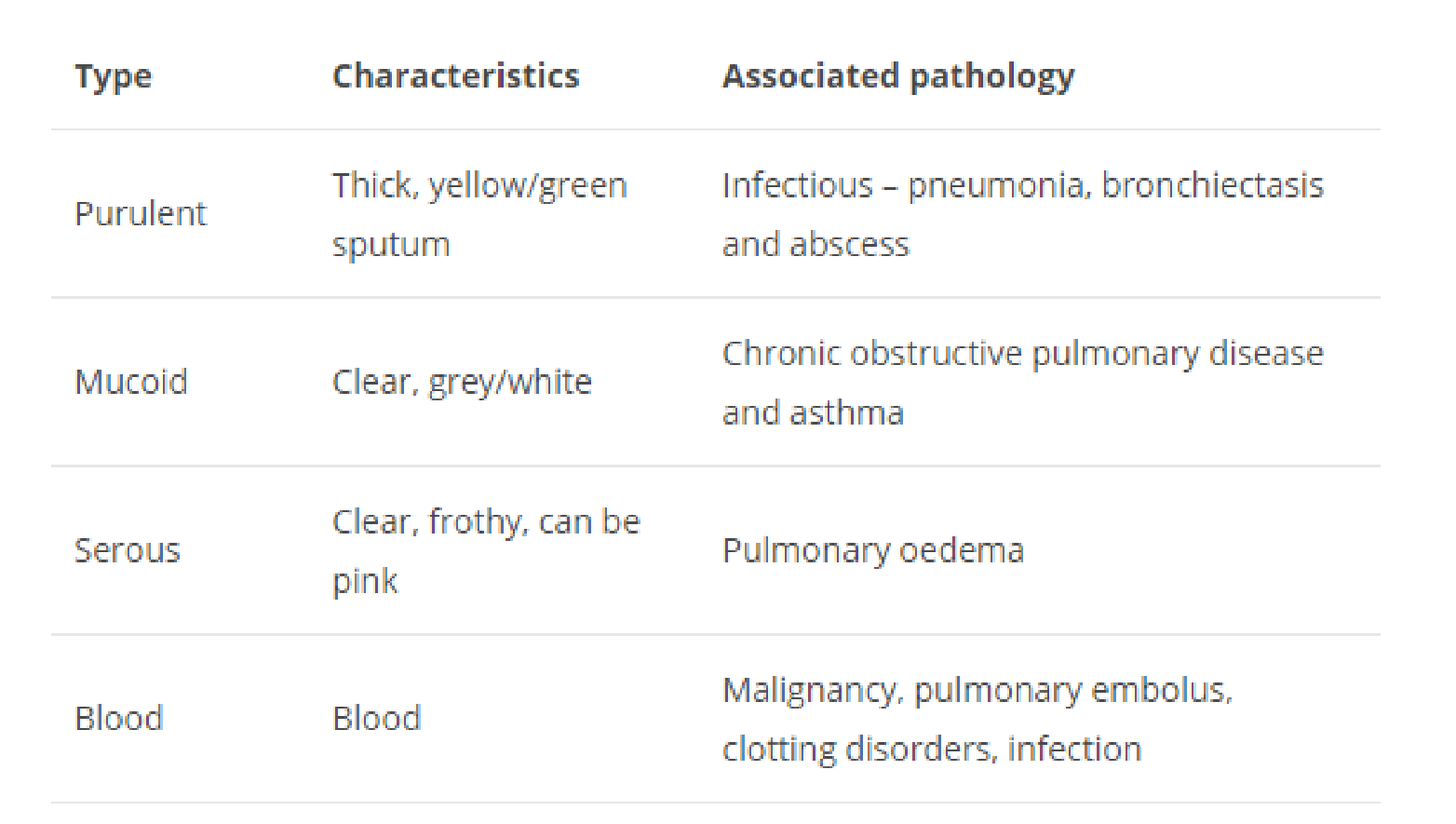
Sputum
Sputum can have many colors and consistency, and these can help define certain conditions.
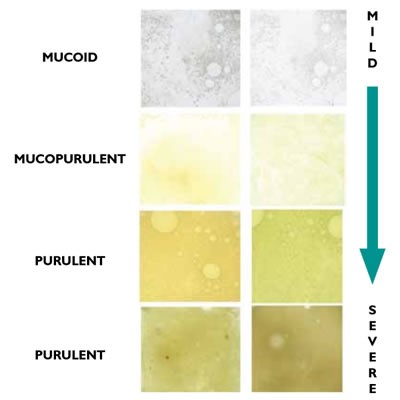 mucous: white or colorless and clear (slimy) mucopurulent: yellowish and cloudy (slimy-purulent) purulent: yellow-greenish and opaque (purulent)
mucous: white or colorless and clear (slimy) mucopurulent: yellowish and cloudy (slimy-purulent) purulent: yellow-greenish and opaque (purulent)
The more yellow the color of the sputum, the higher the addition of pus (pus), i.e. of disintegrating granulocytes.
For example:
Clear sputum: Clear sputum is usually normal, although it may be increased in some lung diseases.
White or gray sputum: White or grayish tinged sputum can also be normal, but may be present in increased amounts with some lung diseases or precede other color changes associated with other conditions.
Dark yellow/green sputum: A type of white blood cells known as neutrophils have a green color to them. These types of white blood cells are attracted to the scene of bacterial infections, and therefore bacterial infections of the lower respiratory tract, such as pneumonia, may result in the production of green sputum. yellow-green sputum is common with cystic fibrosis as well.
Brown sputum: Brown sputum due to the presence of tar, is sometimes found in people who smoke. Sputum may also appear brown or black due to the presence of old blood. Brown sputum is also common with “black lung disease.” These diseases, called pneumoconioses, occur from inhaling substances like coal into the lungs.
Pink sputum: Pink, especially frothy pink sputum may come from pulmonary edema, a condition in which fluid and small amounts of blood leak from capillaries into the alveoli of the lungs. Pulmonary edema is often a complication of congestive heart failure. Pink or blood-tinged sputum is commonly caused by tuberculosis worldwide.
Bloody sputum: Bloody sputum, even just a trace of blood tinged sputum, should always be evaluated. Coughing up blood (hemoptysis) can be serious, and is the first sign of lung cancer in 7 to 35 percent of people. Bloody sputum may also occur with a pulmonary embolism, a condition in which a blood clot in the leg breaks off and travels to the lungs. Even 1 teaspoon to 2 teaspoons of coughed up blood is considered a medical emergency, and coughing up a fourth of a cup of blood is considered massive hemoptysis and carries a poor prognosis.
 13.
13.
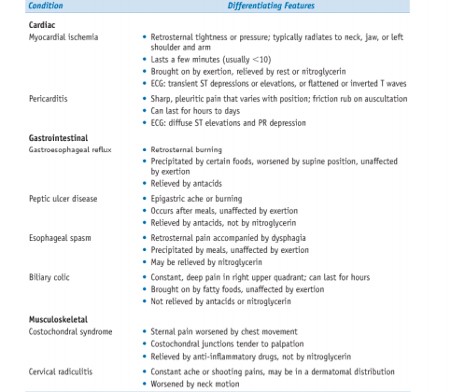
Chest pain.
Angina pectoris.
Type 1; In chronic Ischemic heart disease
Stable (typical) angina:
- Most common form of angina
- caused by an imbalance in coronary perfusion (due to chronic stenosing coronary atherosclerosis) relative to myocardial demand, such as that produced by physical activity, emotional excitement or psychological stress
- variously described as a deep, poorly localised pressure, squeezing, or burning
sensation (like indigestion), but unusually as pain
- relieved by rest (decreasing demand) or administering vasodilators, such as nitroglycerin and calcium channel blockers (increasing perfusion)
Prinzmetal variant angina
- uncommon form of episodic myocardial ischemia
- caused by coronary artery spasm
- Pathogenesis: individuals with Prinzmetal variant angina may have significant coronary atherosclerosis —> but anginal attacks are unrelated to physical activity, heart rate, or
blood pressure
- Prinzmetal angina generally responds promptly to vasodilators
Type 2; in acute coronary syndrome
Unstable or crescendo angina
- refers to a pattern of increasingly frequent, prolonged (>20 min), or severe angina or chest discomfort ● sudden onset angina
- described as frank pain, precipitated by progressively lower levels of physical activity or even occurring at rest
- more severe and lasts longer than chronic stable angina
- Pathogenesis: caused by the disruption of an atherosclerotic plaque with superimposed partial thrombosis and possibly embolisation or vasospasm (or both) (lecture: results
from atherosclerotic plaque disruption and repair)
- one-half of patients with unstable angina have evidence of myocardial necrosis; for others, acute MI may be imminent
Differential diagnosis
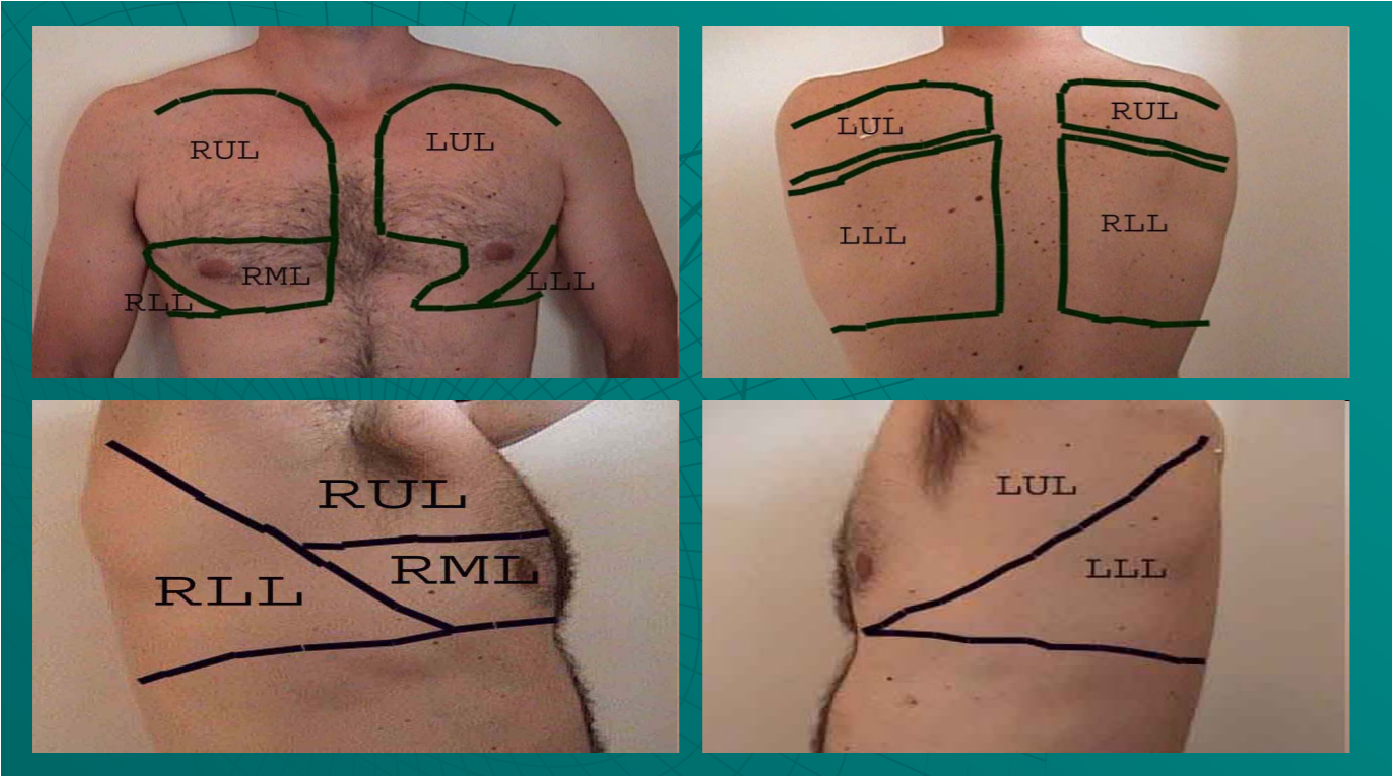
14. Inspection of the chest, pathological chest deformities
PHYSICAL EXAMINATION
1. Inspection
- Skin color
 Neck vein distention ● Extremities – clubbing etc.
Neck vein distention ● Extremities – clubbing etc.
2. Examination of chest wall
- AP / Lateral ratio
- Barrel chest vs. Funnel breast
- Pectus Carinatum (“Pigeon Breast”)
- Kyphosis
- Scoliosis
- Kyphoscoliosis
PATHOLOGICAL CHEST DEFORMITIES
Pectus excavatum
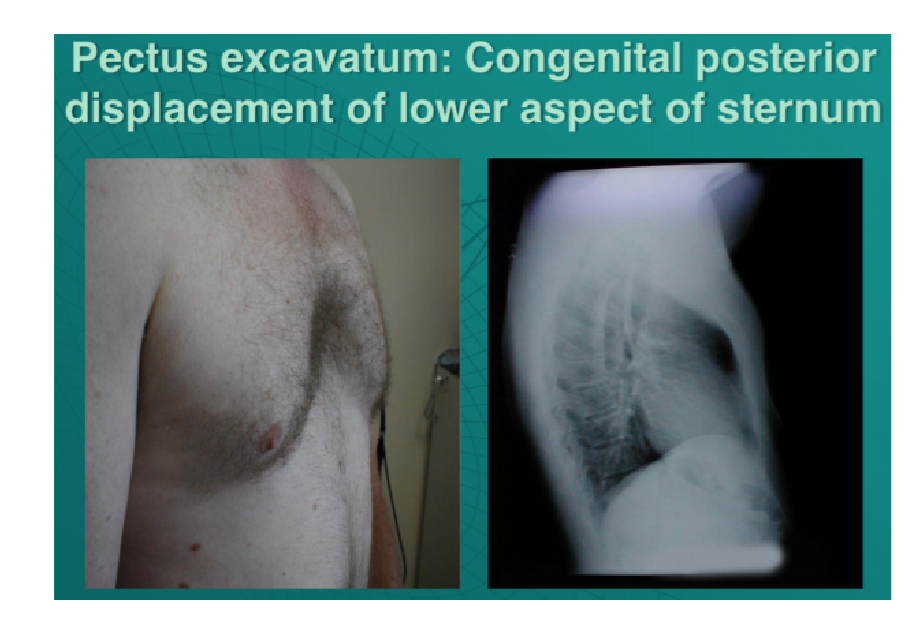 Congenital deformity of the anterior thoracic wall in which the sternum and rib cage are shaped abnormally
Congenital deformity of the anterior thoracic wall in which the sternum and rib cage are shaped abnormally- Due to too much growth of the connective tissue that joins the ribs to the breastbone which causes sternum to grow inwards
- This produces a caved-in or sunken appearance of the chest
- Can impair cardiac and respiratory function and cause pain in the chest and back
Barrel chest
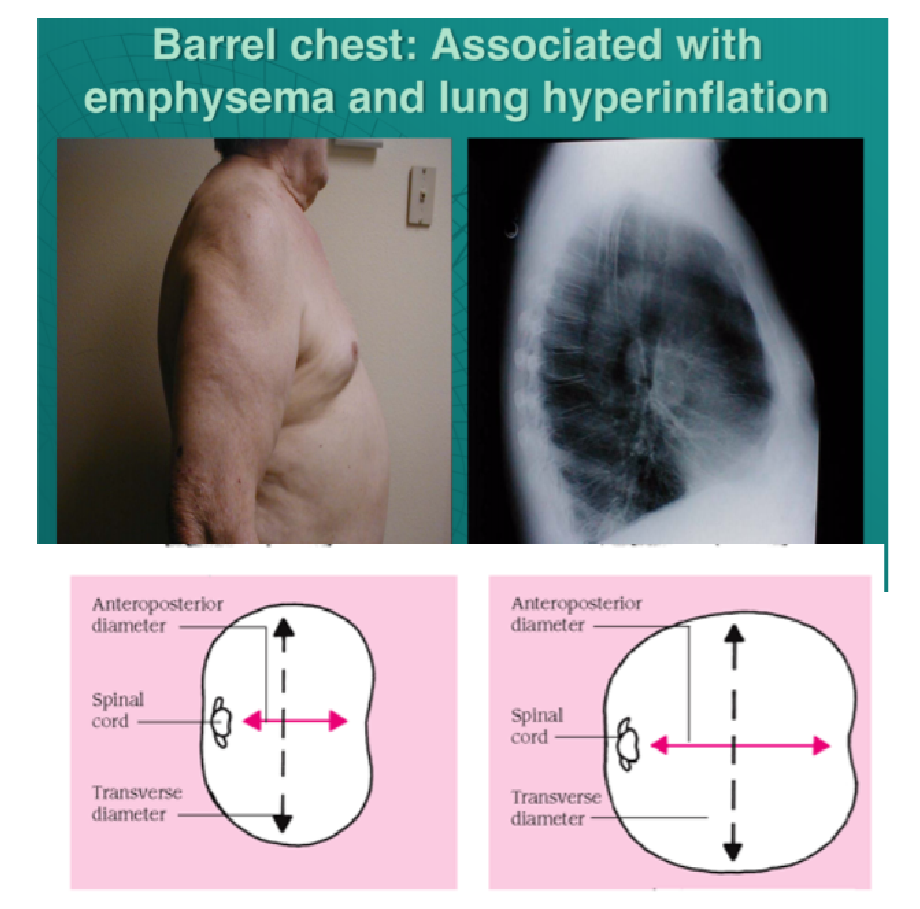 Ratio of anteroposterior to transverse diameter is 1:1 (normal is 1:2)
Ratio of anteroposterior to transverse diameter is 1:1 (normal is 1:2)- Occurs because lungs are chronically overinflated forcing the rib cage to stay expanded for long periods of time – most often
associated with emphysema (as it occurs in
COPD)
- Can also occur in older people: ribs may angle outward at the joints where they attach to the spine and become fixed in their most expanded position
- May be more pronounced in older adults who also have an exaggerated, forward rounding of the back (kyphosis)
Kyphosis
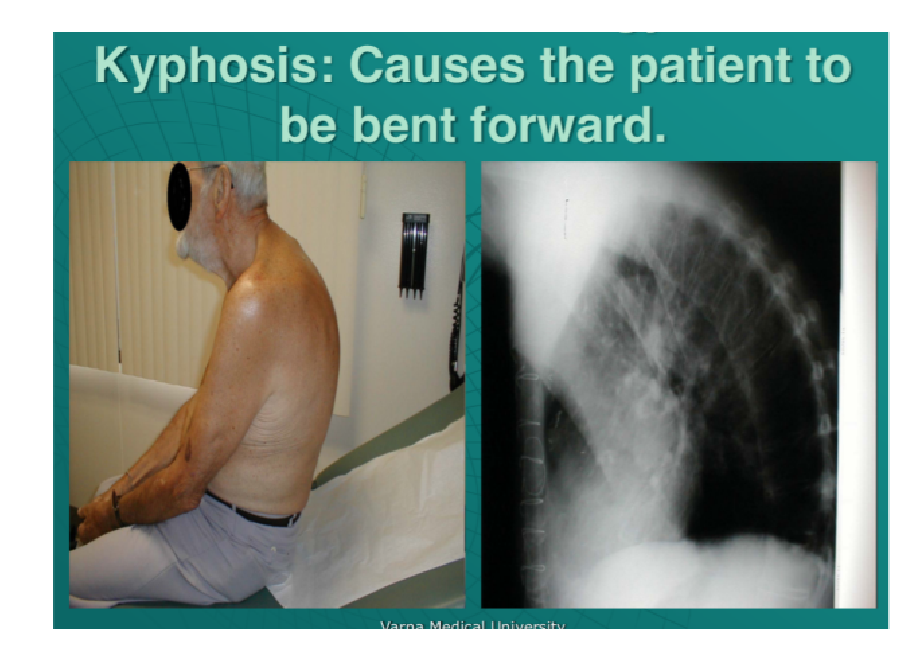 Exaggerated curvature of the upper (thoracic) spine that creates a hunchback appearance
Exaggerated curvature of the upper (thoracic) spine that creates a hunchback appearance- It can result from developmental problems, poor posture, degenerative diseases (such as arthritis), osteoporosis with compression fractures of the vertebrae, and trauma to the spine
- Can affect people of any age
15. Palpation of the chest- pathologic changes.
 Inspection
Inspection
- Thorax: Symmetry, shape ● Respiratory frequency:
– normal (14-20 breaths/min.), tachypnoe (> 20/min) shallow breathing, bradypnoe (<14/min), hyperpnea (>20/min) deep breathing
- Rhythm of respiration: regular, irregular (Insp/Expiration: ratio 1:2)
- Determination of the pulmonary border
 Palpation of the chest
Palpation of the chest
- Patient in gown—>chest accessible & exposed
- Explore painful &/or abnormally appearing areas
- Chest expansion – position hands as below, have patient inhale deeply —> hands lift out laterally
Palpation- Assessing Fremitus
- Fremitus = normal vibratory sensation with palpating hand when patient speaks • Place ulnar aspect (pinky side) of hand firmly against chest wall
- Ask patient to say “Boy”
- You’ll feel a transmitted vibratory sensation —> fremitus!
- Assess posteriorly & anteriorly (i.e. lower & upper lobes)
- * Not Performed in the absence of abnormal findings *
Fremitus – Pathophysiology:
- Increased w/consolidation (e.g. pneumonia)
- Decreased in absence of air filled lung tissue (e.g. effusion).
16. Percussion of the lungs – principles, normal and pathological finding
Percussion of the chest involves listening to the volume and pitch of percussion notes across the chest to identify underlying pathology. Correct technique is essential to generating effective percussion notes. Percussion is an assessment technique which produces sounds by the examiner tapping on the patient’s chest wall. Just as lightly tapping on a container with your hands produces various sounds, so tapping on the chest wall produces sounds based on the amount of air in the lungs. Percussion sets the chest wall and underlying tissues into motion, producing audible sounds and palpable vibrations. Percussion helps to determine whether the underlying tissues are filled with air, fluid, or solid material.
Percussing the anterior chest is most easily done with the patient lying supine; the patient should sit when percussing the posterior chest. Place the first part of the middle finger of your nondominant hand firmly on the patient’s skin. Then, strike the finger placed on the patient’s skin with the end of the middle finger of your dominant hand. Watch a video segment of percussion technique.
Work from the top part of the chest downward, comparing sounds heard on both the right and left sides of the chest. Visualize the structures underneath as you proceed.
Percussion technique
- Place your non-dominant hand on the patient’s chest wall.
- Position your middle finger over the area you want to percuss, firmly pressed against the chest wall.
- With your dominant hand’s middle finger, strike the middle phalanx of your non-dominant hand’s middle finger using a swinging movement of the wrist.
- The striking finger should be removed quickly, otherwise, you may muffle the resulting percussion note.
Areas to percuss
Percuss the following areas of the chest, comparing side to side as you progress (see image example below):
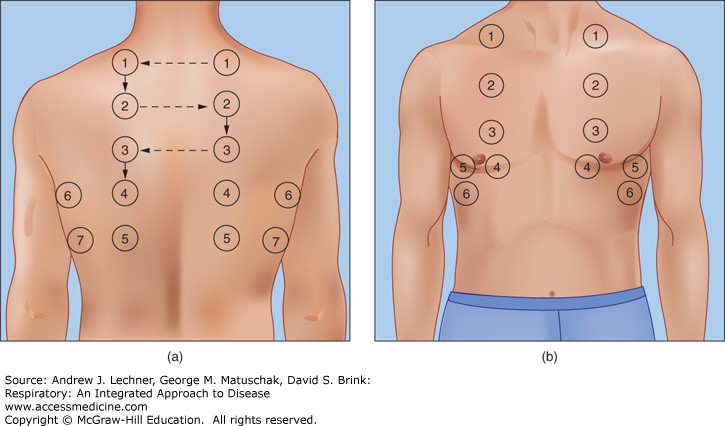 Supraclavicular region: lung apices
Supraclavicular region: lung apices- Infraclavicular region
- Chest wall: percuss over
3-4 locations bilaterally
- Axilla
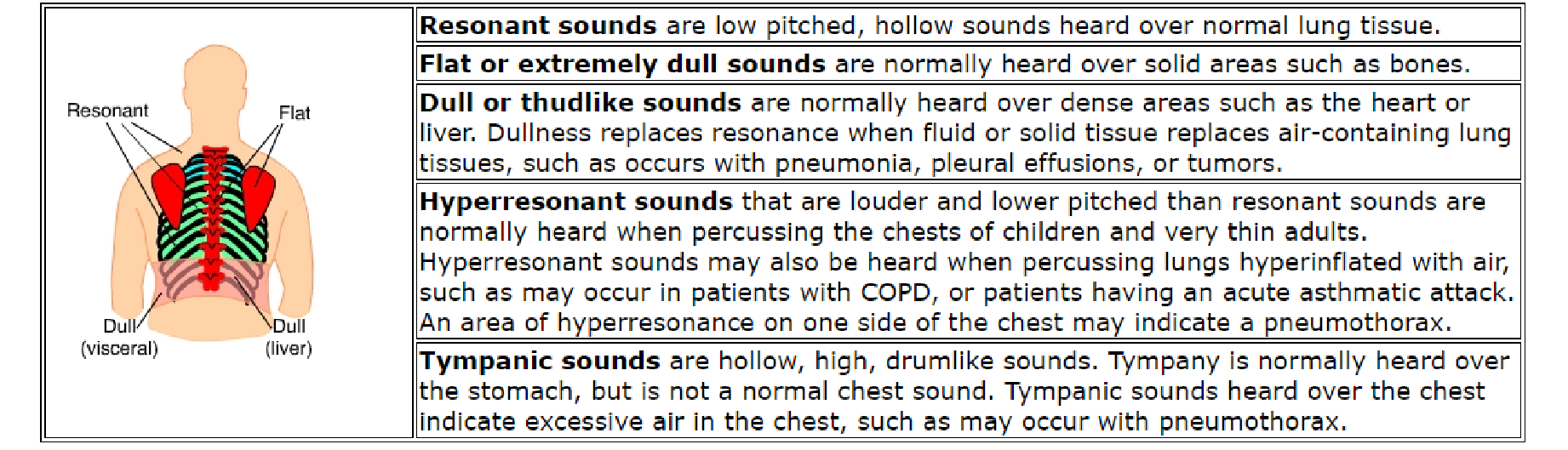
Types of percussion note
- Resonant: a normal finding (listen to the example in the video demonstration).
- Dullness: suggests increased tissue density (e.g. cardiac dullness, consolidation, tumour, lobar collapse).
- Stony dullness: typically caused by an underlying pleural effusion.
- Hyper-resonance: the opposite of dullness, suggestive of decreased tissue density (e.g. pneumothorax).
Pathological changes
Causes of Dullness:
- Fluid outside of lung (effusion)
- Fluid or soft tissue filling parenchyma (e.g. pneumonia, tumor)
Causes of hyper- resonance:
- COPD—> air trapping
- Pneumothorax (air filling pleural space)
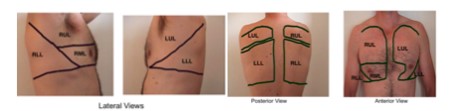
17. Auscultation of the lungs – types of breathing and mechanism of formation adventitious sounds
Auscultation:
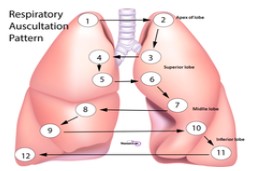 The main auscultations points of the lungs at the patient’s back (image); The lung tips are always being auscultated from ventral!!!!
The main auscultations points of the lungs at the patient’s back (image); The lung tips are always being auscultated from ventral!!!!
Breathing noise (pathologic)
- Stridor: Stenosis of respiratory tract or obstructive pulmonary disease
- Dry rattle noises: ex: wheeze inflammation and mucus of the upper airways 3. Wet rattle noise: liquid in the alveoli and bronchial tree, pneumonia
- Wet rattle noise: liquid in the alveoli and bronchial
tree, pneumonia
Bronchial Breath Sounds:
Heard normally when listening over the trachea. If consolidation (e.g. severe pneumonia) upper airway sounds transmitted to periphery & apparent upon auscultation over the affected area.
Absence of Sound: In chronic severe emphysema, often small tidal volumes & thus little air movement.
– Also w/very severe asthma attack, effusions, pneumothorax
Egophony: in the setting of suspected consolidation, ask the patient to say “eee” while auscultating. Normally, it sounds like “eee”..
- Listening over consolidated area generates a nasally “aaay” sound.
- Not a common finding (but interesting)
Types of breathing and mechanism of formation
• Hyperpnea
definition: Hyperpnea is increased depth and rate of breathing
may be physiologic—as when required to meet metabolic demand of body tissues (for example, during or after exercise, or when the body lacks oxygen at high altitude or as a result of anemia) it may be pathologic, as when sepsis is severe
• Kussmaul breathing
- rate/variable
- deep laboured breathing pattern • is a form of hyperventilation (more respirations to decrease CO2) • association
– diabetic ketoacidosis (DKA), uremia, metabolic acidos – pneumonia
• Cheyne- Stokes
abnormal pattern of breathing
—> progressively deeper, and sometimes faster, breathing followed by a gradual decrease that results in a temporary stop in breathing (apnea). —> pattern repeats, each cycle = 30 seconds to 2 minutes long association / clinical occurrence
- normal – during sleep in children and aged
- various pathologies
 heart failure / left
heart failure / left- brain damage
- increased intracerebral pressure secondary to numerous causes
- drug induced respiratory depression
• Biot’s respirations
• abnormal pattern of breathing characterised by groups of quick, shallow inspirations followed by regular or irregular periods of apnea • associations/ clinical occurrence:
- damage to the pons due to strokes or trauma or by pressure on the pons due to uncal or tentorial herniation.
- can be caused by opioid use
Adventitious sounds
| Crackles (Rales) | Wheezes and Rhonchi |
| Discontinuous | Continous |
| Intermittent, nonmusical and brief | >250msec, musical, prolonged |
| Fine crackles: soft, high-pitched, brief (5-10msec) | Wheezes: high pitched (>400Hz) with hissing or shrilling |
| Coarse crackles; low pitch and brief (20-30msec) | Rhonchi; relatively low-pitched (<200Hz) snoring quality |
Characteristic breath sounds
| Duration of sounds | Intensity of
expiratory sound | Pitch of expiratory sound | Location where heard normally | |
| Vesicular | Inspiratory sounds last longer than
expiratory ones | Soft | Relatively low | Over most of both lungs |
| Bronchovesi cular | Inspiratory and expiratory sounds are about equal | Intermediate | Intermediate | Often in the 1st and 2nd interspaces anteriorly and between the scapulae |
| Bronchial | Expiratory sounds last longer than
inspiratory ones | Loud | Relatively high | Over the manubrium, if heard at all |
| Tracheal | Inspiratory and expiratory sounds are about equal | Very loud | Relatively high | Over the trachea in the
neck |
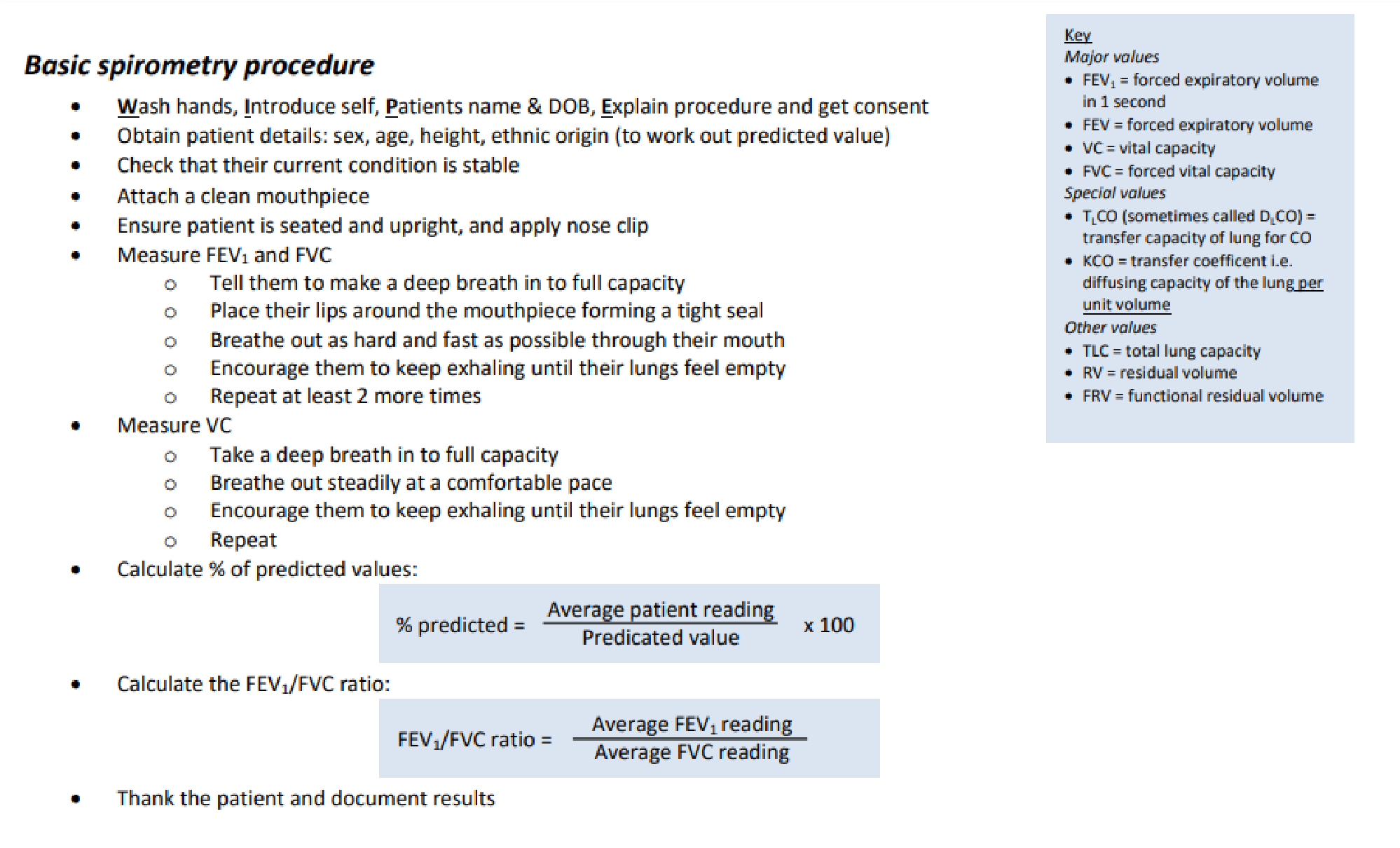
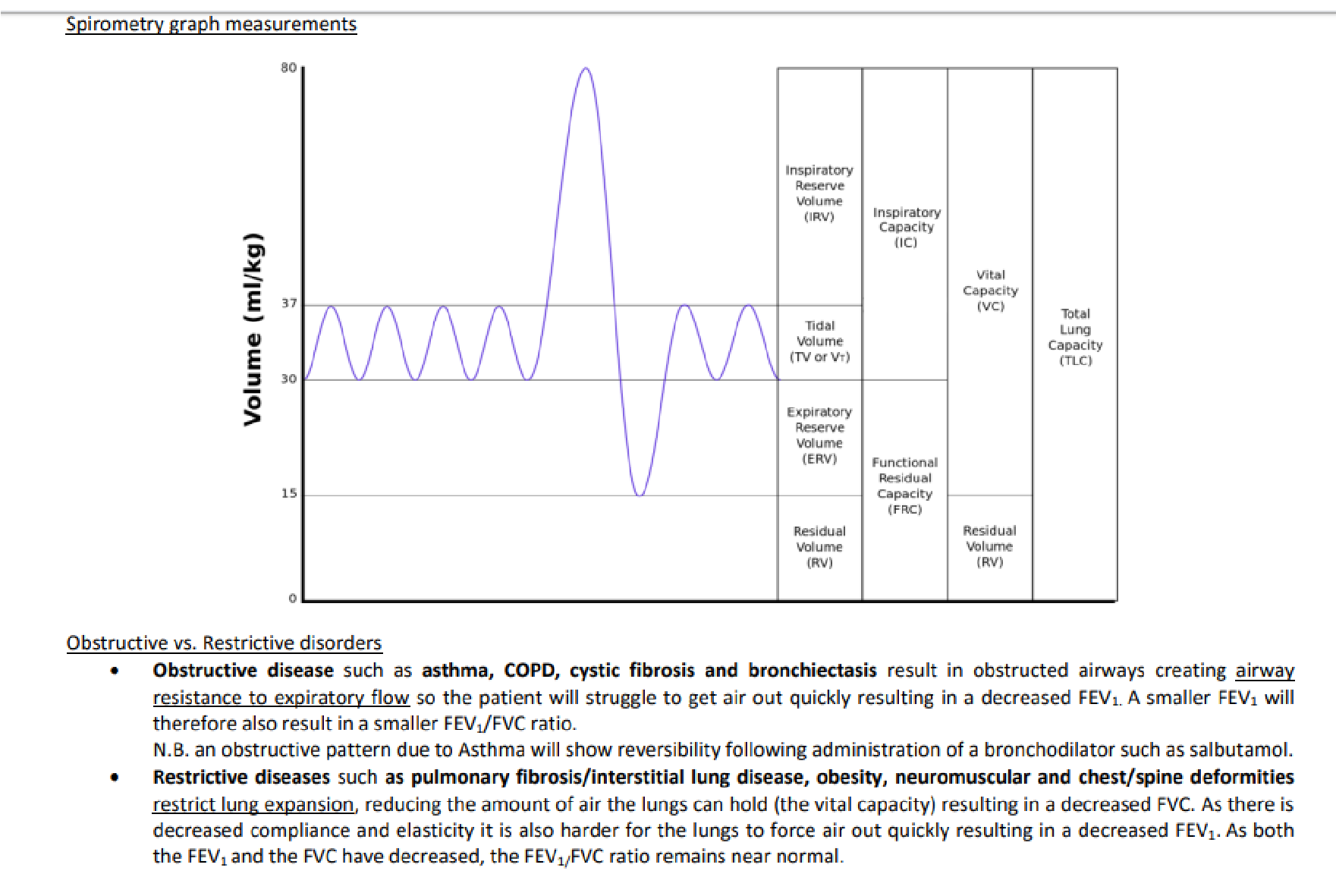
18. Spirometry test and blood gas analysis. Changes in lung diseases
General information about lung volumes/ capacities
Lung/Pulmonary volumes and capacities
- Tidal volume (TV or ) = is the air breathed in and out during normal respiration (0,5L)
- Inspiratory reserve volume (IRV) = additional air that can be breathed in after normal inhalation ( 3L)
- Inspiratory capacity (IC) = TV + IRV = 3,5 L
- Expiratory reserve volume (ERV) = additional air that can be breathed out after normal exhalation (1,1L)
- Residual volume (RV) = the air left in the lungs after most forceful (max.) expiration(1,2L)
- Vital capacity (VC) = TV+IRV+ERV = 4,6 L
- Total lung capacity (TLC) = VC+RV = 5,8 L
- Functional residual capacity (FRC) = is the amount of air that remains in the lungs in the end of normal expiration = ERV + RV = 2,3 L
;’<1%#=(“’$0(’=($”#0(+’>&’”?*01=(-(0″
Minute respiratory volume (MRV) is the total amount of new air moved into the respiratory passages per minute
- Minute respiratory volume: tidal volume x respiratory rate per min
- normal : 0,5L x 12 breaths per min = 6L/min
Alveolar ventilation (AV) is the total volume of new air entering the alveoli each minute
- maximal voluntary ventilation (MVV): 120-170 L/min
- these areas include alveoli, alveolar sacs, alveolar ducts and respiratory bronchioles AV per minute = f x (TV-DS) unit: L/min f= respiratory frequency (12-14 breaths/min) at rest DS=dead space
TV= tidal volume Respiratory diseases to classify respiratory diseases as either restrictive or obstructive, FVC and FEV1 are measured during the “Tiffeneau-test” by making use of a diagnostic tool, the spirometer. In the tiffeneau test, the patient is asked to exhale as quickly as possible after maximum
inhalation. The time and exhaled volume are measured:
- FVC (forced vital capacity): is the fastest, forcibly expelled expiratory volume
- FEV1 (forced expiratory volume in 1 sec): is the amount of gas (volume) that can forcibly and maximally be expelled during the1st sec of exhalation.
;’@10=$%%&’*-A”’3B5’1C’-/(’)*-$%’D$?$D*-&’E<FG
With the “Tiffeneau test” mainly obstructive ventilation disorders can be diagnosed, since the test gives information about the respiratory tracts resistance. The increase in respiratory tract resistance leads to a decrease in FEV1.
Arterial blood gas. https://geekymedics.com/arterial-blood-gas-sampling/
Blood gases provide important clinical information for patients with respiratory disorders, compromised circulation, or abnormal metabolism.The amount of oxygen and carbon dioxide in the blood can be sampled and reported as the partial pressure of the gas. Blood gas analysis also typically includes a direct measurement of the serum pH and estimates of serum bicarbonate derived from the measured partial pressure of carbon dioxide (Pco2) and pH. Current tests often include other useful information such as direct measurement of lactic acid as lactate, total hemoglobin, and serum electrolytes.
An arterial blood sample is the reference standard for pH, oxygen, carbon dioxide, and lactate content providing a description of the oxygen and carbon dioxide content of the blood after leaving the pulmonary circulation and before any gas exchange in the peripheral tissues has occurred. In scenarios that require precise determination of these variables, an arterial sample is necessary.
Arterial blood gas samples are sometimes used for evaluation of serum hemoglobin and electrolytes. Blood gas analyzers typically have good concordance with the reference laboratory autoanalyzer; however, there may be clinically significant variances depending on the equipment involved, especially for sodium, hemoglobin, and chloride. Results should be interpreted with caution when they are significantly abnormal.
Normal ranges
- pH: 7.35 – 7.45
- PaCO2: 4.7 – 6.0 kPa || 35.2 – 45 mmHg
- PaO2: 11 – 13 kPa || 82.5 – 97.5 mmHg
- HCO3–: 22 – 26 mEq/L
- Base excess (BE): -2 to +2 mmol/L
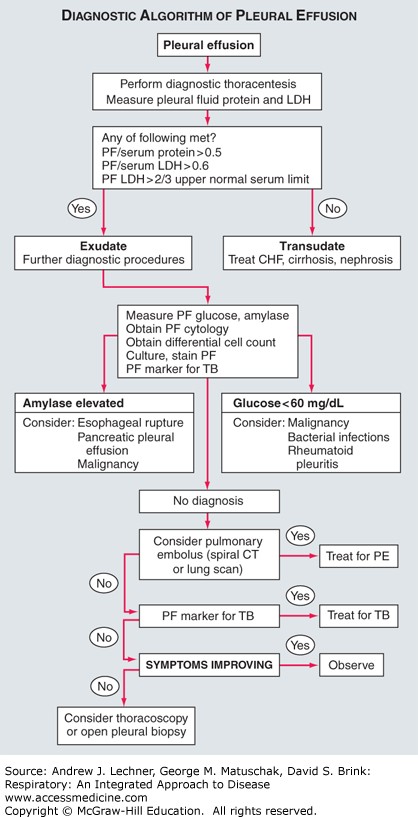
19. Thoracocentesis . Analysis of the pleural effusion.
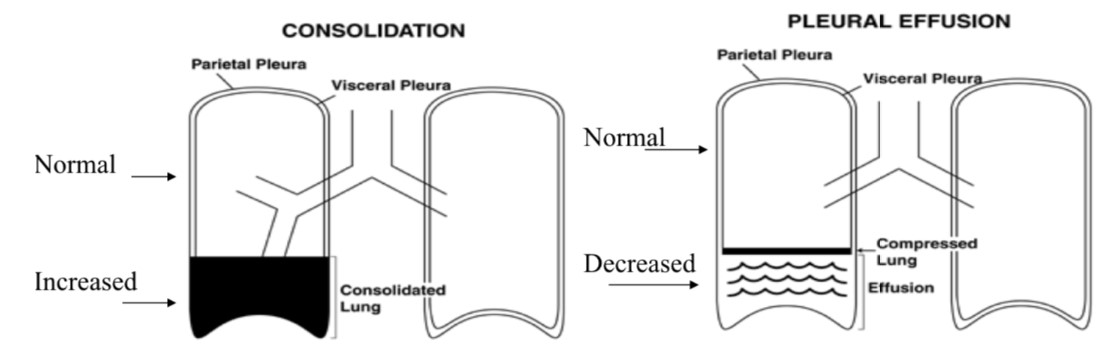
 The pleural space is a potential space between the juxtaposed visceral pleura covering the outer surface of the lung and parietal pleura lining the inner surface of the chest wall.
The pleural space is a potential space between the juxtaposed visceral pleura covering the outer surface of the lung and parietal pleura lining the inner surface of the chest wall.- normally it contains a few milliliters of fluid. Laboratory characteristics of normal pleural fluid include:
- pH = 7.6,
- H?01-(*,I’J’K9L’MN+O’E)”’?%$”=$’H?01-(*,I’P’7’MN+OG6’
- HM%#D1″(I’P’?%$”=$’HM%#D1″(I6’
- [lactate dehydrogenase] <50% of plasma [LDH].
- The number of WBC is <1,000/mL and consists mainly of mononuclear cells with a few erythrocytes and mesothelial cells.
- Normally there are <10 mL of pleural fluid in the entire thoracic space of a healthy adult.
Physiology of the Pleural Space
- The normal hydrostatic pressure of ~30 mm Hg in systemic capillaries of the parietal pleura drives extravasation of ultrafiltrate into the pleural space. Due to hydrostatic pressure exceeding the net colloid osmotic pressure gradient of ~24 mm Hg between those systemic capillaries and the few proteins in normal pleural space fluid.
- At the same time, the normally low hydrostatic pressure of ~12 mm Hg within pulmonary capillaries lying beneath the visceral pleura is considerably less than this same colloid osmotic pressure gradient of 24 mm Hg between the plasma and normal pleural fluid.
- This osmotic gradient thus drives pleural fluids into the lung tissue, adding to pulmonary lymph created within all of the alveoli.
- By this mechanism, as long as the protein concentration within the pleural space remains low and/or pulmonary capillary pressure is normal, virtually all of the fluid being lost from systemic capillaries into the pleural space is rapidly removed into the lungs across the visceral pleural membrane to form lymph.
Transudate and Exudate
- But extravasated fluids accumulate into a pleural effusion if increased capillary hydrostatic pressures overwhelm the osmotic pressure gradient, as in systemic or pulmonary hypertension. A pleural effusion created by such altered hydrostatic forces would be considered a transudate.
- Pleural fluid also accumulates if the colloid osmotic pressure within the pleural space becomes elevated, as by neoplasm or infectious agent. Such an increase in pleural fluid osmotic pressure reduces the normally large osmotic gradient between plasma proteins and proteins within the pleural space. A pleural effusion created under such conditions would be classified as an exudate, and may become empyemic.
- Effusions of either type will accumulate when lymphatic obstruction/other defect prevents their drainage or reabsorption. Additional sources of pleural fluid include excessive drainage of lymph from the interstitial spaces of the lung into the visceral pleura, or ascites fluid from the peritoneal cavity that enters the thoracic space via small holes in the diaphragm.
Laboratory Analysis of Pleural Fluids
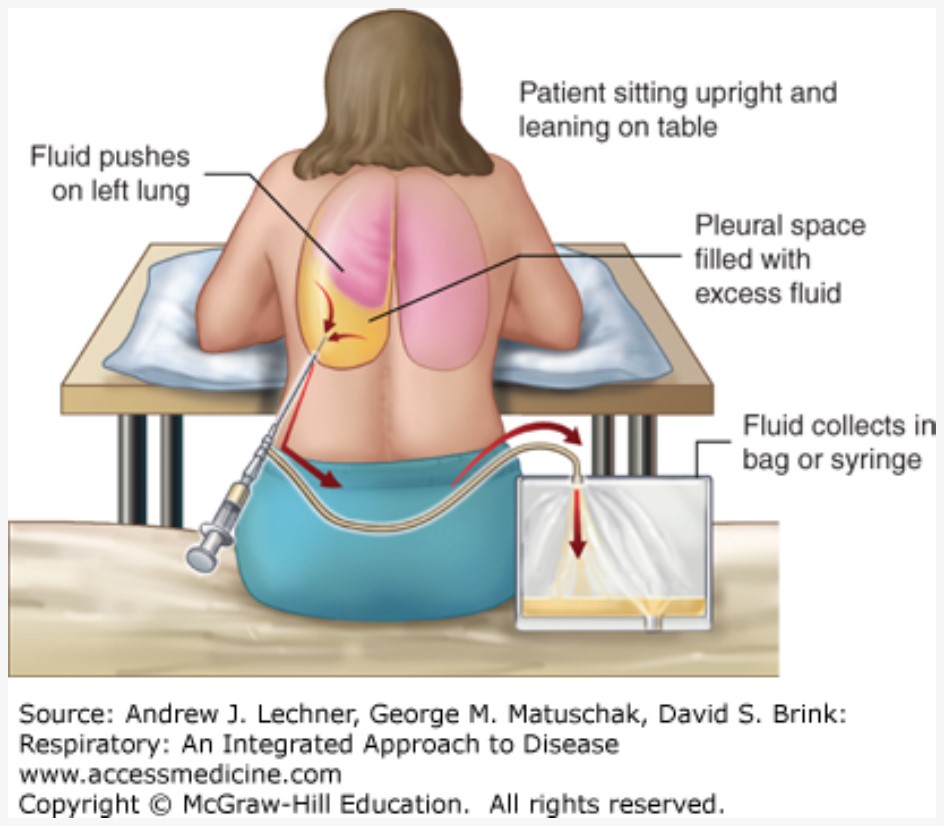 Thoracentesis is the intentional and guided collection of pleural fluid from the otherwise closed chest, a procedure that may yield several liters depending on the cause of a patient’s effusion.
Thoracentesis is the intentional and guided collection of pleural fluid from the otherwise closed chest, a procedure that may yield several liters depending on the cause of a patient’s effusion.- Has both diagnostic and therapeutic values, since evacuating effusions may remove infectious material and permit re-expansion of lung lobes that develop atelectasis by fluid compression.
- Proper technique for handling pleural effusions includes sending all fluid obtained.
- Specimens are sent to flow cytometry when lymphoma or leukemia is suspected.
- First step in its evaluation is to determine whether the fluid is a transudate or an exudate. Often the physician will have a strong suspicion.
- Transudates is present in: congestive heart failure; cirrhosis with ascites; nephrotic syndrome when resulting in hypoproteinemia; recent peritoneal dialysis; myxedema in patients with hypothyroidism; acute lobar atelectasis due to multiple causes; constrictive pericarditis; superior vena caval obstruction; and pulmonary embolism.
- Exudates are caused by local factors that create abnormal pleural fluids or obstruct their reabsorption, often in the presence of free or adherent cells. Normal leukocytes that are commonly found in exudates include resident lung macrophages and lymphocytes, as well as neutrophils recruited by chemokines and microbial secretions. Their intrapleural release of cytokines and other inflammatory mediators augments the local concentration of high molecular weight proteins. This increase in intrapleural colloid osmotic pressure retards fluid reabsorption into the lung lymphatics, in addition to whatever primary immunomodulatory effects these mediators induce.
- Abnormal host cells that are commonly associated with exudates include many neoplastic forms that represent primary thoracic tumors or metastases to the pleural compartment.
- Exudates may need extensive testing to establish their etiologies, diseases in which they may develop:
- Pneumonias of nearly all types
- Neoplasms, either primary or secondary
- Pulmonary embolism
 Sarcoidosis and other connective tissue diseases
Sarcoidosis and other connective tissue diseases- Hematogenously spread systemic infections
- Chylothorax
- Postmyocardial infarction syndrome
- Asbestosis
- Meigs syndrome (a benign ovarian tumor producing ascites)
- Pancreatic disease ● Uremia
- Chronic atelectasis
- Adverse drug reaction
Distinguishing between Transudates and Exudates
The two most useful criteria for identifying an effusion as an exudate or transudate are its [LDH] and total [protein]. Acknowledging the role of [protein] on pleural colloid osmotic pressure, an exudate is defined by at least one of the three following criteria:
- Pleural fluid [protein]/serum [protein] >0.5
- Pleural fluid [LDH]/serum [LDH] >0.6
- Pleural fluid [LDH] >200 IU/L, or >2/3 normal upper limit for serum
Depending upon the outcomes of these initial evaluations, other useful testing includes:
- Pleural fluid specific gravity, >1.016 in exudates
- Pleural fluid [cholesterol], >60 mg/dL in exudates
- Pleural fluid fibrinogen, seen in exudates and potentially indicating a clot
- Pleural fluid number of WBCs, >1,000/µL in exudates
- Pleural fluid number of RBCs, > 100,000/µL in exudates (including malignancy, pulmonary embolism/infarction, or trauma)
- Pleural fluid [bilirubin]/serum [bilirubin], >0.6 g/dL in exudates ● Pleural fluid [amylase] or its activity, elevated in some types of exudates
20. Arterial hypertension, blood pressure measurement.
Normal arterial blood pressure
- Normal is the BP with no excess CV mortality
- Hypotension< 90< 60
- Normal 90 – 120 over 60 – 80 Arterial Hypertension
- Prehypertension 121 – 139 over 81 – 89
- Stage 1 Hypertension 140 – 159 over 90 – 99 Q’R-$M(’L’S&?(0-(,”*1,T’KUB’10’T’KBB
- High BP is the strongest risk factor for CV mortality
Blood pressure measurement Specific BP concepts and terms
- Systolic Hypertension
- Diastolic Hypertension
- Abnormal Pulse Pressure
- Inequality of BP in Both Arms Orthostatic Hypotension
- White-coat hypertension
Blood pressure measurements
- At the office
- At home
- Holter BP monitoring
- During exercise – hypertensive reaction
Techniques for BP measurement
- Correct cuff size
- Bag = 80% arm circumference
- Width
- Cuff Errors
- too narrow
- too short
- Blood pressure technique
- On the initial patient visit, the blood pressure should be taken in each arm. The usual position is with the patient sitting. The position should be noted with the blood pressure obtained.Blood pressure should also be taken with the patient standing and lying down.
- To begin, deflate the blood pressure cuff completely by opening the stopcock attached to the rubber bulb of the sphygmomano-meter.
- Wrap the cuff firmly around the upper arm leaving at least 3 cm clear above the antecubital fossa.
- Palpate the patient’s radial pulse, close the stopcock and inflate the cuff until the pulse is no longer palpable. The pressure when the pulse is no longer palpable approximates the systolic blood pressure.
- Deflate the cuff and note the pressure level at which pulse re-appears again approximately the systolic pressure.
- Place the stethoscope bell on the medial aspect of the antecubital fossa at the site of the brachial artery.
- Inflate the cuff again to a pressure 20 mm above the approximated systolic pressure. Deflate the cuff slowly until the first sound is heard. This is the SYSTOLIC BLOOD PRESSURE by auscultation.
NOTE: In some patients, the sound may DISAPPEAR completely at a pressure below the systolic blood pressure and then reappear as the cuff pressure continues to drop. This is known as the AUSCULTATORY GAP. Its presence should be noted when recording the blood pressure.—> related to carotid atherosclerosis and increased arterial stiffness in hypertensive patients
- Continue to deflate the cuff and note the point where the sound becomes muffled. RECORD THIS VALUE.
- i. if the sound is muffled, continue to deflate the cuff and note the pressure at which the sound disappears completely. This pressure should be recorded as the probable diastolic blood pressure.
- Repeat on the other arm.
- BP should have 3 readings plus auscultatory gap.
- Auscultatory Gap
- Review How to Chart BP
- Non-vanishing sound to zero mm. Hg.
a. Significance 1. thyrotoxicosis
- aortic regurgitation
- miscellaneous
7. Normal arterial blood pressure
- diurnal variation
- normal range 8. Systolic Hypertension
- Diastolic Hypertension
- Normal Pulse Pressure 11. Abnormal Pulse Pressure
- widened
- narrowed
12. Inequality of BP in Both Arms
a. causes
13. Orthostatic Hypotension
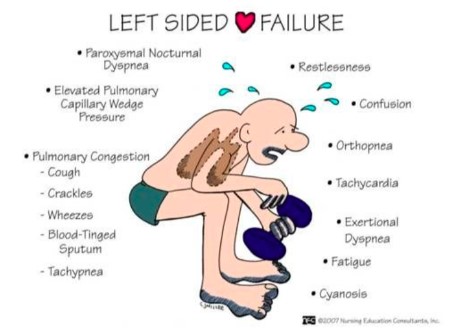
21. Clinical manifestations and types of left-sided heart failure.
| Left–sided heart failure | Fluid may back up in your lungs, causing shortness of breath. |
| Right–sided heart failure | Fluid may back up into your abdomen, legs and feet, causing swelling. |
Types
There are two types of left-sided heart failure. Drug treatments are different for the two types
- Heart failure with reduced ejection fraction (HFrEF), also called systolic failure:
The left ventricle loses its ability to contract normally. The heart can’t pump with
enough force to push enough blood into circulation.
- Heart failure with preserved ejection fraction (HFpEF), also called diastolic failure
(or diastolic dysfunction): The left ventricle loses its ability to relax normally (because the muscle has become stiff). The heart can’t properly fill with blood during the resting period between each beat.
Causes:
- ischemic heart disease
- systemic hypertension
- aortic and mitral valvular disease
- myocardial disease – cardiomyopathy, myocarditis
Diabetes
Obesity
Sleep apnea
- loss of muscle due to poison: alcohol, cobalt, doxorubicin
- rhythm disturbances (e.g. tachyarrhythmia)
Diagnosis
- Cardiac catheterisation
- Echocardiogram
- Electrocardiogram (EKG)
- Electrophysiology study: This test records the heart’s electrical activities and pathways. It can help find what’s causing heart rhythm problems and identify the best treatment.
- Radionuclide imaging (thallium stress test): This non-invasive procedure can identify if there is severe heart damage. A radioactive isotope is injected into a vein and a special camera or scanner records how it travels through the heart. Any heart damage can be plotted, locating the damaged area of the heart. This procedure can be done with an electrocardiogram, during both rest and exercise.
- Treadmill Exercise Test with Peak V02: This test measures a patient’s capacity to exercise and the amount of oxygen the heart provides muscles during the test. Results reveal the severity of the left-sided heart failure and helps provide a prognosis.
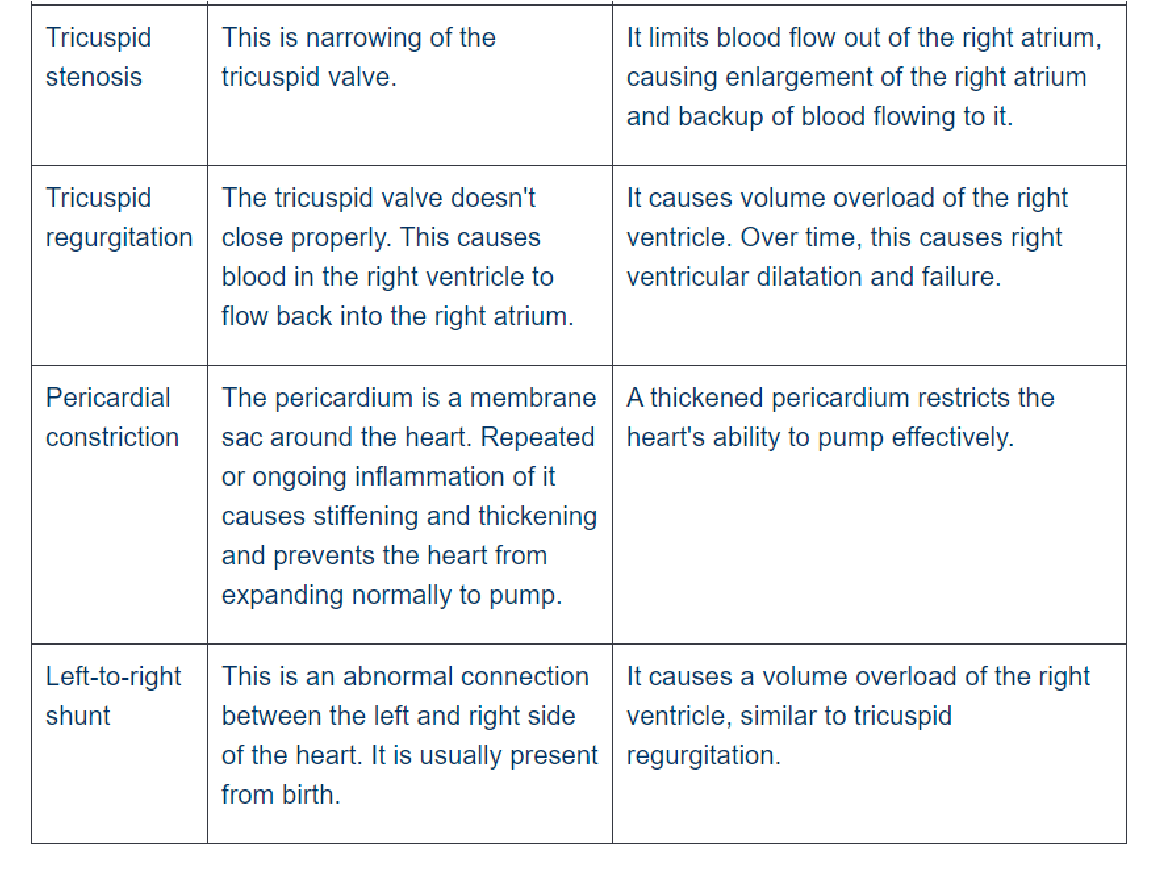
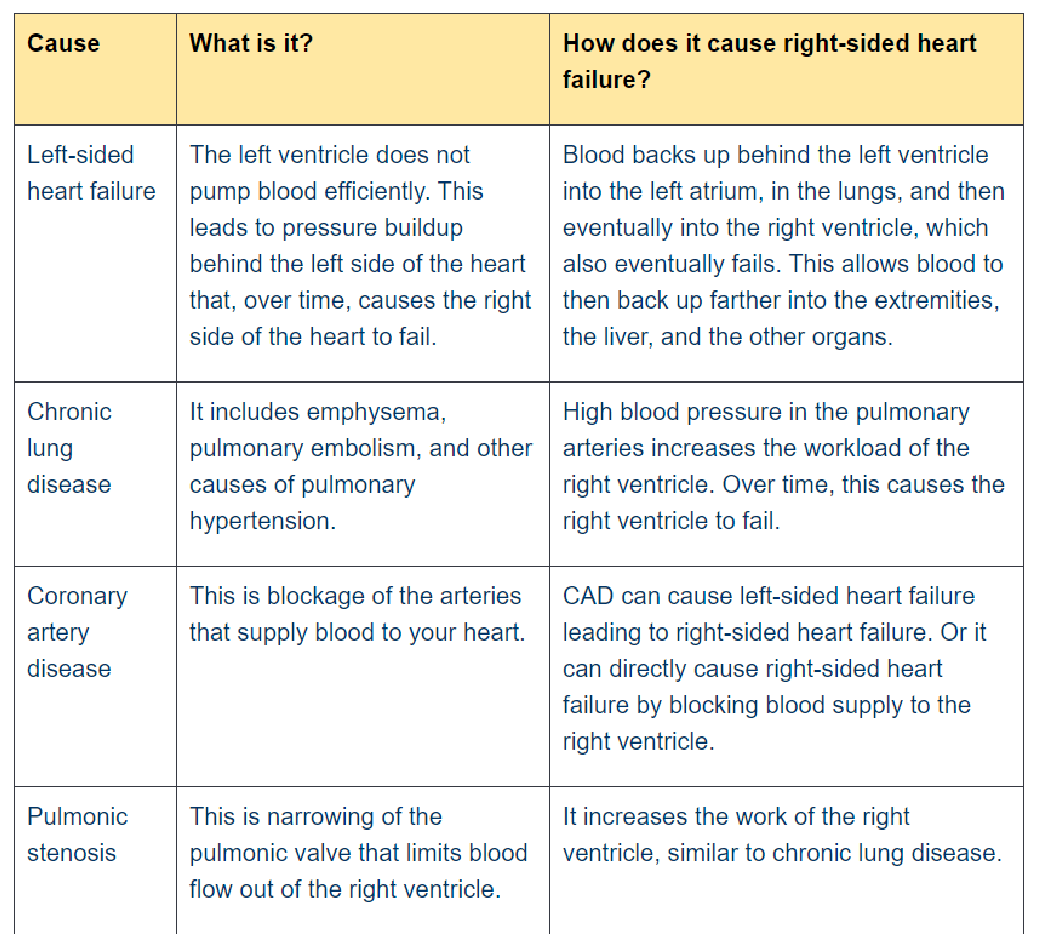
22. Clinical manifestations and types of right sided heart failure
Right-sided heart failure means that the right side of the heart is not pumping blood to the lungs as well as normal. Occurs when the right ventricle has difficulty pumping blood to your lungs. Blood backs up in your blood vessels, which causes fluid retention in your lower extremities, abdomen, and other vital organs. It is also called cor pulmonale or pulmonary heart disease
CAUSES
- Consequence of left-sided heart failure
- Cor pulmonale in which right heart failure occurs due to intrinsic lung disease
- Pulmonary or tricuspid valvular diseases
- Pulmonary hypertension secondary to pulmonary thromboembolism (coronary artery diseases)
- Myocardial disease affecting the right heart
- Congenital heart disease with left-to-right shunt
CLINICAL MANIFESTATIONS
- Tricuspid or pulmonary valvular disease
- Distention of neck veins (raised jugular venous pressure—> engorgement visualised)
- Tender, enlarged, palpable congested liver (nutmeg liver) and spleen (if both: hepatosplenomegaly) —> raised pressure in inferior vena cava reflects back into liver´s venous system
- Renal hypoxia—> subcutaneous peripheral edema, especially pitting edema of the ankles due to raised pressure in small venules and capillaries of the lower limb supplemented by gravity
- Increased pressure in their lumen with transudation of fluid into interstitial tissues
=> pleural effusion, ascites, hydrothorax Diagnosis
DIAGNOSIS ● Blood tests:
- type natriuretic peptide (BNP) or N-terminal pro-BNP—measure the concentration of a hormone produced by the left ventricle
- Metabolic panel—to check for electrolyte imbalance, kidney failure (since symptoms of kidney disease are similar to those of CHF) and liver disease
- Complete blood count (CBC)—to check for anemia, which can cause similar symptoms to CHF as well as contribute to CHF
- Thyroid tests—these tests check the level of thyroid hormone in the blood; both hyperthyroidism (too much thyroid hormone) and hypothyroidism (too little thyroid hormone) can cause heart failure
- Galectin-3 and ST2 are tests that measure the levels of these proteins in blood. Elevated levels of these biomarkers may be used to indicate if a person with heart failure is at increased risk for complications and needs more aggressive treatment
23. Premature beats, supraventricular tachycardias
Premature beat:
A ventricular premature beat is an extra heartbeat resulting from abnormal electrical activation originating in the ventricles before a normal heartbeat would occur. They are common, particularly among older people.
- May be caused by physical/emotional stress, intake of caffeine or alcohol, or use of cold or hay fever remedies with drugs that stimulate the heart, such as pseudoephedrine.
- Other causes are coronary artery disease (especially during or shortly after a heart attack) and disorders that cause ventricles to enlarge, i.e. heart failure and heart valve disorders.
Symptoms
- Isolated ventricular premature beats have little effect on the pumping action of the heart and usually do not cause symptoms, unless they are extremely frequent.
- The main symptom is the perception of a strong or skipped beat (palpitations).
- Ventricular premature beats are not dangerous for people who do not have a heart disorder.
- However, frequently in people who have a structural heart disorder, they may be followed by more dangerous arrhythmias such as ventricular tachycardia or ventricular fibrillation, which can cause sudden death.
Diagnosis: Electrocardiography Treatment:
- Lifestyle changes
- Sometimes beta-blockers
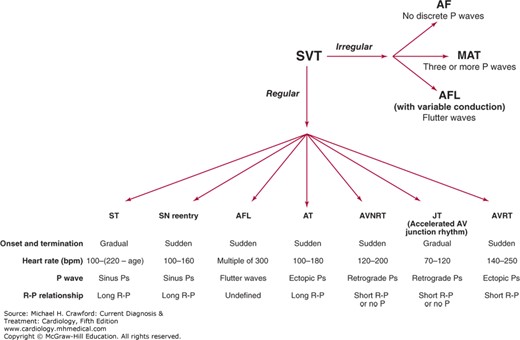
Supraventricular tachycardias (SVTs)
SVT are rapid rhythm disturbances originating from the atria or the atrioventricular (AV) node.
- In the absence of a bundle branch block, there is intact conduction to the ventricles via the right and left bundles leading to a narrow and normal-appearing QRS.
- Therefore, these arrhythmias are also often called narrow complex tachycardias.
- Because many of the SVTs are episodic, many clinicians also refer to this group of arrhythmias as paroxysmal SVTs.
- Radiofrequency ablation has become an important therapeutic option in the management of SVTs because of its ability to cure these arrhythmias safely.
Pathophysiology & Etiology
Tachyarrhythmias occur as a result of three main mechanisms: reentry, which is most common; enhanced or abnormal automaticity; and triggered activity.
- Reentrant arrhythmias sustain themselves by repetitively following a revolving pathway comprising two limbs, one that takes the impulse away from and one that carries it back to the site of origin.
- For reentry to exist, an area of slow conduction must occur, and each limb must have a different refractory period. In this situation, pacing (by inducing refractoriness in one limb of the circuit) can initiate a reentrant tachycardia. Once established, pacing can also terminate the tachycardia by interfering with impulse propagation in one of the limbs.
- Automaticity = refers to spontaneous and, often, repetitive firing from a single focus, which may either be ectopic or may originate in the sinus node.
- This mechanism comprises two subcategories:
- Enhanced automaticity is a focus that fires spontaneously and may originate in the sinus node, subsidiary pacemakers in the atrium including the Eustachian ridge, Bachmann bundle, coronary sinus and AV valves, the AV node, His-Purkinje system, and the ventricles.
- Abnormal automaticity is secondary to a disease process causing alterations in ionic flow that produces a less negative resting diastolic membrane potential. Threshold potential is therefore more easily attained, thereby increasing the probability of a sustained arrhythmia.
- Triggered arrhythmias = depend on oscillations in the membrane potential that closely follow an action potential. In the absence of new external electrical stimulus, oscillations/ after-depolarizations, cause new action potentials to develop. Thus, each new action potential results from the previous action potential.
- These arrhythmias are produced by early or late after-depolarization, depending on the timing of the first after-depolarization relative to the preceding action potential (the one that spawned the triggered activity).
- In early after-depolarizations, membrane repolarization is incomplete, allows an action potential to be initiated by a subthreshold stimulus. This is associated with electrolyte disturbance and may be the mechanism responsible for arrhythmogenesis related to the prolonged QT syndrome and torsades de pointes caused by quinidine. – With delayed after-depolarization, membrane repolarization is complete, but an
abnormal intracellular calcium load causes spontaneous depolarization. The reason for the high calcium levels is unclear, but may be related to inhibition of the sodium pump by drugs such as digoxin. In either type of arrhythmia, the process may be repetitive and lead to a sustained tachycardia.
ESSENTIALS OF DIAGNOSIS
● Heart rate greater than 100 bpm at rest. ● Rhythm is supraventricular in origin
24. Atrial fibrillation and flutter
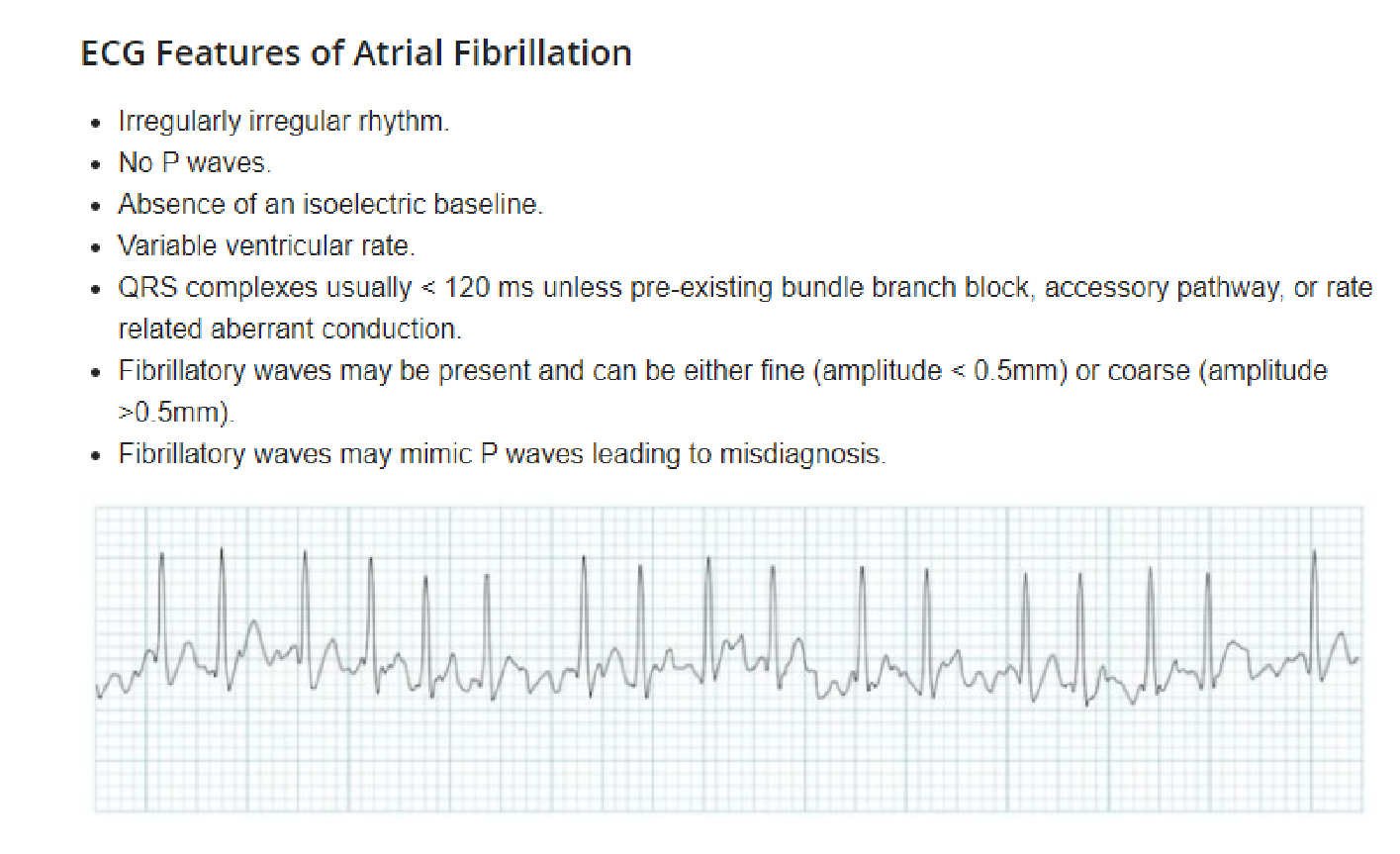 In atrial fibrillation, the heart’s upper chambers (atria) contract randomly and sometimes so fast that the heart muscle cannot relax properly between contractions. This reduces the heart’s efficiency and performance. Atrial fibrillation happens when abnormal electrical impulses suddenly start firing in the atria.
In atrial fibrillation, the heart’s upper chambers (atria) contract randomly and sometimes so fast that the heart muscle cannot relax properly between contractions. This reduces the heart’s efficiency and performance. Atrial fibrillation happens when abnormal electrical impulses suddenly start firing in the atria.
Atrial fibrillation (Afib) is a commonly seen type of supraventricular tachyarrhythmia that is characterized by uncoordinated atrial activation resulting in an irregular ventricular response. While the exact mechanisms are still poorly understood, associations with a number of cardiac (e.g., valvular heart disease, coronary artery disease) and noncardiac (e.g., hyperthyroidism, electrolyte imbalances) risk factors have been established. Individuals with Afib are typically asymptomatic. However, when symptoms do occur, these usually include palpitations, lightheadedness, and shortness of breath. Physical examination typically reveals an irregularly irregular pulse. Ineffective atrial emptying as a result of Afib can lead to stagnation of blood and clot formation in the atria, which in turn increases the risk of stroke and other thromboembolic complications. The diagnosis is confirmed by an ECG showing indiscernible P waves and a narrow QRS complex with irregular QRS intervals.
Echocardiography is used in patients with Afib to rule out structural heart disease and detect the presence of atrial thrombi.
Classification of Atrial Fibrillation
Classification is dependent on the presentation and duration of atrial fibrillation as below:
- First episode – initial detection of AF regardless of symptoms or duration
- Recurrent AF – More than 2 episodes of AF
- Paroxysmal AF – Self terminating episode < 7 days
- Persistent AF – Not self terminating, duration > 7 days
- Long-standing persistent AF – > 1 year
- Permanent (Accepted) AF – Duration > 1 yr in which rhythm control interventions are not pursued or are unsuccessful
Atrial flutter is another type of commonly seen supraventricular tachyarrhythmia that is usually caused by a single macroreentrant rhythm within the atria. The risk factors for atrial flutter are similar to those of Afib. In atrial flutter, the atrial rate is slower than in Afib and the ventricular rhythm is usually regular. Treatment is similar to that of Afib, consisting of anticoagulation and strategies to control heart rate and rhythm. Atrial flutter frequently degenerates into atrial fibrillation.
Atrial_fibrillation#xid=GS0Baf&anker=Z7874fab08b9e0e4a88f584ee2bdad121
25. Disturbances in conducting system of the the heart (Heart Blocks)
Arrhythmias can be classified by rate (normal, tachy, brady), or mechanism (automaticity, reentry, fibrillation) or by origin:
Atrial: premature atrial contractions, wandering atrial pacemaker, multifocal atrial tachycardia, atrial flutter, atrial fibrillation
Junctional arrhythmias: Supraventricular tachycardia, AV nodal reentrant tachycardia most common cause of Paroxysmal supra-ventricular tachycardia, junctional rhythm, junctional tachycardia, premature junctional complex.
Atrio-ventricular: AV reentrant tachycardia occurs when a re-entry circuit crosses between the atria and ventricles somewhere other than the AV node; Wolff-Parkinson-White syndrome, Lown-Ganong-Levine syndrome.
Ventricular: Premature ventricular contractions, accelerated idioventricular rhythm, monomorphic ventricular tachycardia, ventricular fibrillation
Bradyarrhythmias; Sinus bradycardia, Coronary sinus rhythm, junctional rhythm, idioventricular rhythm, agonal rhythm, complete heart block, ventricular asystole
Tachyarrhythmias: Sinus tachycardia, Supraventricular tachycardia, atrial flutter, atrial fibrillation, multifocal atrial tachycardia or chaotic atrial rhythm, accelerated idioventricular rhythm, ventricular tachycardia, ventricular fibrillation.
Heart blocks
AV blocks; common cause of bradycardia.
1st degree heart block= prolonged PR
2nd degree heart block
– Type 1 Second degree heart block= Mobitz 1 (Wenckebach phenomenon) -Type 2 second degree heart block= Mobitz 2
3rd degree is a complete heart block
SADS- sudden arrhythmic death syndrome
CAD
Viral myocarditis, Brugada syndrome, long QT syndrome, Catecholaminergic polymorphic ventricular tachycardia, hypertrophic cardiomyopathy
1st degree AV block:
PR>200ms. No specific hemodynamic disturbance or specific treatment required.
Causes of blocks; Increased vagal tone, inferior MI, mitral valve surgery, myocarditis, hyperkalemia, AV node blocking drugs; beta blockers, calcium channel blockers. Symptomatic patients are treated with atropine. 2nd degree AV block, Mobitz 1
Progressive prolongation of PR into a non-conducted P wave. The PR interval is longest immediately before the dropped beat. The PR after the dropped beat is the shortest. Commonly 3:2, 4:3, 5:4

PP is constant. RR shortens progressively. AV node cells progressively fatigue until they fail to conduct an impulse.
2nd degree AV block Mobitz 2
Intermittent non-conducted P waves without prolongation of PR interval. PR is constant and may be prolonged. Atrial impulses are blocked sporadically. Can be 2:1, 3:1

3rd degree AV block; complete block
No conduction through the AV node.
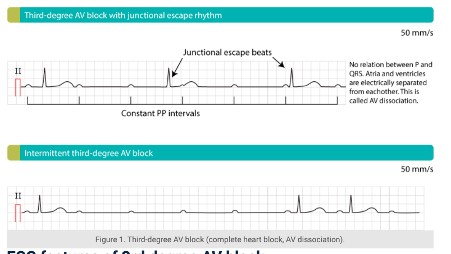 Will cause cardiac arrest. Regular ventricular rhythm and varying PR interval suggest third degree block as atrial and ventricular rates are not equal (shown as PR varying).
Will cause cardiac arrest. Regular ventricular rhythm and varying PR interval suggest third degree block as atrial and ventricular rates are not equal (shown as PR varying).
26. Auscultation of the heart. Mechanisms of formation of heart sounds
AUSCULTATION OF THE HEART
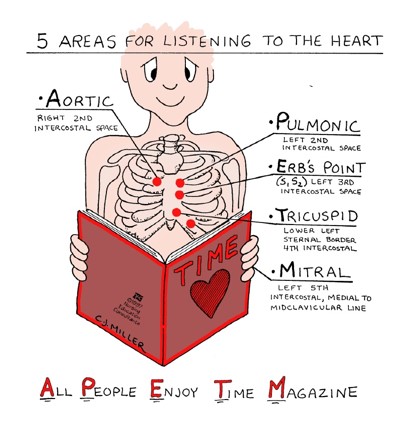 CARDIAC CYCLE
CARDIAC CYCLE
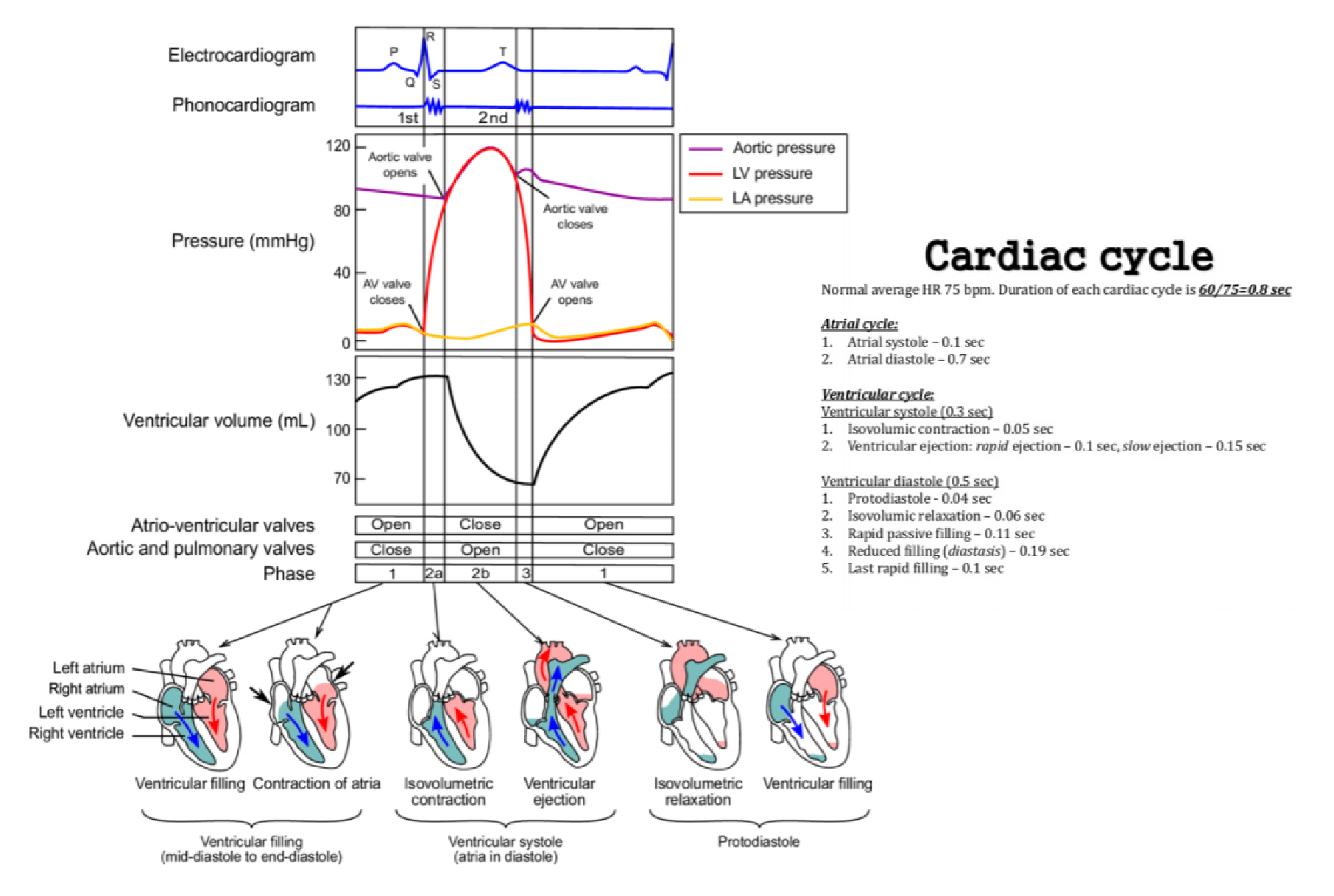
HEART SOUNDS
= acceleration and deceleration of blood
Normal heart sound: (Lub-dub)
- The “ lub” is the first heart sound, commonly termed S1, and is caused by turbulence caused by the closure of mitral and tricuspid valves at the start of systole
- The second sound, “dub” or S2, is caused by the closure of aortic and pulmonic valves, marking the end of systole. Thus the time period elapsing between the first heart sound and second sound defines systole (ventricular ejection) and the time between the second sound and the following first sound defines diastole (ventricular filling).
- 3rd heart sound: at rapid filling period of diastole —> The gallop associated with early diastolic filling is the S3 and may be heard pathologically in such states as volume overload and left ventricular systolic dysfunction —> associated with heart failure:
Rapid ventricular filling
- Mitral regurgitation – this is when one of the mitral valve leaflets that usually stop blood flowing from the left ventricle to the left atrium fails, allowing blood into the atria during systole. This means that the left atrium will be overfilled, leading to rapid ventricular filling when the mitral valve opens.
- Elevated left atrial and left ventricular filling pressures, usually a result of a stiffened and dilated left ventricle
- Ventricular septal defect – this is a hole in the wall between the two ventricles, which allows rapid filling from the other ventricle
Poor left ventricular function
- Post-MI – the death of tissue in the ventricular wall due to loss of blood supply causes wall areas which do not move as well as normal (hypokinesia), or not at all (akinesia), meaning they relax more slowly, so the ventricular filling is relatively too rapid.
- Dilated cardiomyopathy – the ventricular walls are abnormal for a variety of reasons, and become thin and stiff so do not relax well. => S3 may be normal in people under 40 years
- The S4 is a late diastolic sound (starts shortly before S1) and may be heard in such pathologic states as uncontrolled hypertension (tachycardia) —> mechanism is not absolutely certain, it is generally accepted that S4 is caused by stiffening of the walls of the ventricles (usually the left), which produces abnormally turbulent flow as the atria contract to force blood into the ventricle
29. Electrocardiography – normal pattern.
- 3 bipolar limb leads; I, II, III
- 3 Augmental unipolar limb leads; avF (looks at inferior) , avR (looks at right side), avL (looks at left side)
- 6 Precordial chest leads; V1-V6
Location:
V1; R. 4th intercostal space parasternal
V2; L. 4th intercostal space parasternal
V4; Mid clavicular 5th intercostal space
V3; Between V2 and V4
V5; Axillary line 5th intercostal space
V6; midaxillary line 5th intercostal space
1. Rate
RR; 4 squares; 300/4=75bpm
300/ no. of squares=HR
1=300bpm
2=300/2=150bpm
3=300/3=100bpm
4=300/4=75
5=300/5=60
6=300/6=50
6 second rhythm strip no. of R waves x 10
10 second rhythm strip no. of R waves x 6
2. Rhythm
RR interval same and regular
3. P wave
Leads II and avR
Sinus rhythm: +ve in II and -ve in avR
No p wave= not sinus; ectopic or junctional
Check PR interval
4. Does every P follow onto a QRS
Determines if there is an AV association. If it does not indicate a heart block.
5. QRS
0.12s
Bunny ears; RBBB
6. ST
Elevation- MI
Inferior infarction; occlusion of R. coronary artery, changes seen in leads II, III, aVF Lateral infarction: occlusion of left circumflex artery, changes seen in leads I, aVL, V5 & V6 Anterior infarction: occlusions of LAD, changes seen V1-V6.
Anterolateral infarction: occlusion of the left main artery; leads I and aVL
Posterior infarction: occlusion of right coronary artery; inversion in anterior leads
7. T wave
T wave inversion=ischemia
Normal values
RR; 50-100bpm/ 0.6-1.2s
P; atrial depolarization; 80ms
PR; Estimate of AV node function; 0.12-0.2s
QRS; ventricular depolarization; 80-120ms/0.12s
J point: end of QRS
ST: 80-120ms
T wave; 160ms
ST interval; 320ms
QT; 300-430ms
PQ; 0.2s

27. Cardiac murmurs – characteristics of cardiac murmurs.
● Heart murmurs result from audible vibrations that are caused by increased turbulence and are defined by their timing within the cardiac cycle.
Causes of Heart Murmurs
- Blood flowing through an abnormal narrowing (e.g. aortic stenosis, mitral stenosis, pulmonary stenosis).
- Blood flowing in the wrong direction through the heart, and mixing with blood flowing in the normal direction (e.g. mitral regurgitation, tricuspid regurgitation).
- An abnormal connection between two different parts of the heart (e.g. atrial septal defect, patent ductus arteriosus). Blood flows across this abnormal connection causing either:
○ Mixing of blood going in different directions
○ Too much blood flowing into another heart chamber
- Blood flowing faster through the heart (e.g. functional murmurs in sepsis and thyrotoxicosis).
Transmitted Heart Murmurs
A structural defect in the heart can result in turbulent blood flow, creating a murmur. Blood flow remains turbulent after it passes across the structural defect and thus the murmur will continue to be heard in the direction that turbulent blood is flowing. Therefore some murmurs are transmitted from the primary structural defect in the direction the blood is flowing.
Examples of murmurs that are transmitted:
- Aortic stenosis – radiates to the carotid arteries
- Mitral regurgitation – radiates to the axilla
When during the cardiac cycle is the murmur heard?
Systole
- Aortic and pulmonary stenosis
- Mitral and tricuspid regurgitation
- Mitral valve prolapse causes a systolic murmur with an opening click
Early diastole
- Aortic and pulmonary regurgitation
Mid/late-diastole
- Mitral and tricuspid stenosis
What are the characteristics of the murmur?
Systolic murmurs
Ejection systolic (crescendo-decrescendo):
- Aortic and pulmonary stenosis Pansystolic:
- Mitral and tricuspid regurgitation
Other causes of ejection systolic murmurs
Aortic sclerosis and hypertrophic obstructive cardiomyopathy (HOCM):
- Both are loudest in the aortic valve area, during expiration
- Aortic stenosis radiates to the carotids, whereas HOCM and aortic sclerosis do not Atrial septal defects and pulmonary stenosis:
- Both are loudest in the pulmonary region
- Atrial septal defects cause wide and fixed splitting of S2 whereas pulmonary stenosis does not
Is the murmur heard loudest using the bell or the diaphragm of the stethoscope?
- High pitched murmurs – Loudest with the diaphragm
- Low pitched murmurs (e.g. mitral regurgitation) – Heard better with the bell
Where is the murmur heard the loudest?
Usually, murmurs are heard loudest in the region of the valve affected.
- Aortic area – 2nd intercostal space right sternal edge
- Pulmonary area – 2nd intercostal space left sternal edge
- Tricuspid area – 4th intercostal space left sternal edge
- Mitral area – Cardiac apex (usually 5th intercostal space in the left midclavicular line)
Do any manoeuvres exaggerate the murmur?
- Aortic valve: Sitting forwards brings the aortic valve closer to the chest wall, thus aortic murmurs are heard louder whilst the patient is sitting forwards.
- Mitral valve: The left lateral decubitus position brings the apex of the heart closer to the chest wall, thus mitral valve murmurs are heard loudest in this position.
Heard loudest on inspiration or expiration?
Inspiration
- During inspiration, the intrathoracic pressure reduces, so more blood flows into the right heart chambers.
- Right-sided valve lesions (pulmonary and tricuspid valves) are therefore loudest during inspiration. Expiration
- During expiration intrathoracic pressure increases, forcing pulmonary vessels to constrict, so blood is forced from pulmonary veins into the left atrium and through the left side of the heart.
- Left-sided heart valve lesions (aortic and mitral valves) are therefore loudest during expiration.
Some murmurs may radiate depending on the direction the turbulent blood flows.
- Aortic stenosis – Radiates to the carotid artery
- Mitral regurgitation – Radiates to the axilla
- Aortic regurgitation – Radiates to the left sternal edge (usually heard best at the left sternal edge and not in the aortic valve region)
- Pulmonary stenosis – Radiates to the left shoulder/infra-clavicular region
Other Important Features on Peripheral Examination
- Pulse character and pulse pressure (the difference between the systolic and diastolic blood pressure)
- Location of apex beat
- Jugular venous pressure (JVP) abnormalities
- Signs of heart failure (e.g. oedema)
28. Examination of the arteries and arterial pulse
Pulse measurement
Sites of palpation
- Carotid
- Brachial
- Radial
- Femoral
- Popliteal
- Posterior tibialis
- Dorsalis pedis
Pulse characteristics
- • Regular or irregular —regularis/irregularis
- • Slow or rapid — frequens/rarus
- • Bounding or shallow — durus/mollis
- • Steep or slow — celer/tardus
- • Full or empty — inanis, vacuus
- • High or small — altus/parvus
- • Equal and non-equal — equalis /inequalis
Technique for palpation of Pulse
With the patient’s hand prone, grasp the patient’s wrist with your fingertips to obtain the radial pulse. Both pulses should be compared to check for differences in rate and amplitude.
The rate is determined by counting for one minute. Ideally the pulse is 72, optimally – 60-80, referent limit – 50-100. Trisection-full pressure until disappearance and maximal release for BP orientation approximately up to 20 mm Hg
Symmetric palpation on both legs and hands for equality of pulses-diminished in PAD.
Grading 1-4 not palpable, barely palpable, palpable, bounding
Pulse measurement upon inspiration-increase in frequency and decrease in amplitude
30. Functional methods of examination of the cardiovascular system youtube.com/watch?v=XU_xeUMJ3Zc
Precordial area and a description of changes to their exact location and character
Data from palpation – point of maximal impulse (PMI) -a description of the normal apical impulse (exact location, width and nature), abnormal apical impulse – in precordium and epigastric. Search fremissman, friction and intense art sounds
Data from percussion – determination of cardiac size and shape of a medium strength percussion.
Dullness (absolute) – normally 2 cm medially from the lMCL in 5th ics .
Flatness(relative) – must be done with a light almost imperceptible percussion (normal size – right border – the left sternal edge, upper – lower edge of the rib IV and then turning arc and coincides with the dullness in theV ics and point of maximal impulse (PMI) in the area).
Data on auscultation – determination of rhythm and heart rate, ratio between heart sounds at the base of the heart and on top of heart, intense tones, splitting of sounds, normal splitting of second heart sound S2-(A2-P2) ones, careful description of the two components of the II tone, additional heart sounds, T3 Gallop and T4 gallop). Murmurs – systolic, diastolic, stenotic or regurgitant, or pericardial rub. NOTE: auscultation also be carried out during normal breathing, in bed, left recumbent position, sitting, standing and squatting. Intensity (loudness) and pitch (frequency) – T1, T3 and T4- low pitched, T2- high pitched. Relation to the S1 and S2 – systolic and diastolic murmurs should be noted – ejection or regurgitation, punctum maximum of murmur (point or area of maximal hearing), duration (early, late), musical characteristics – rough, blowing, and murmur propagation. In search of high pitched murmurs use the membrane of the stethoscope and press harder, but at low frequency – the bell of the stethoscope and presses on the chest.
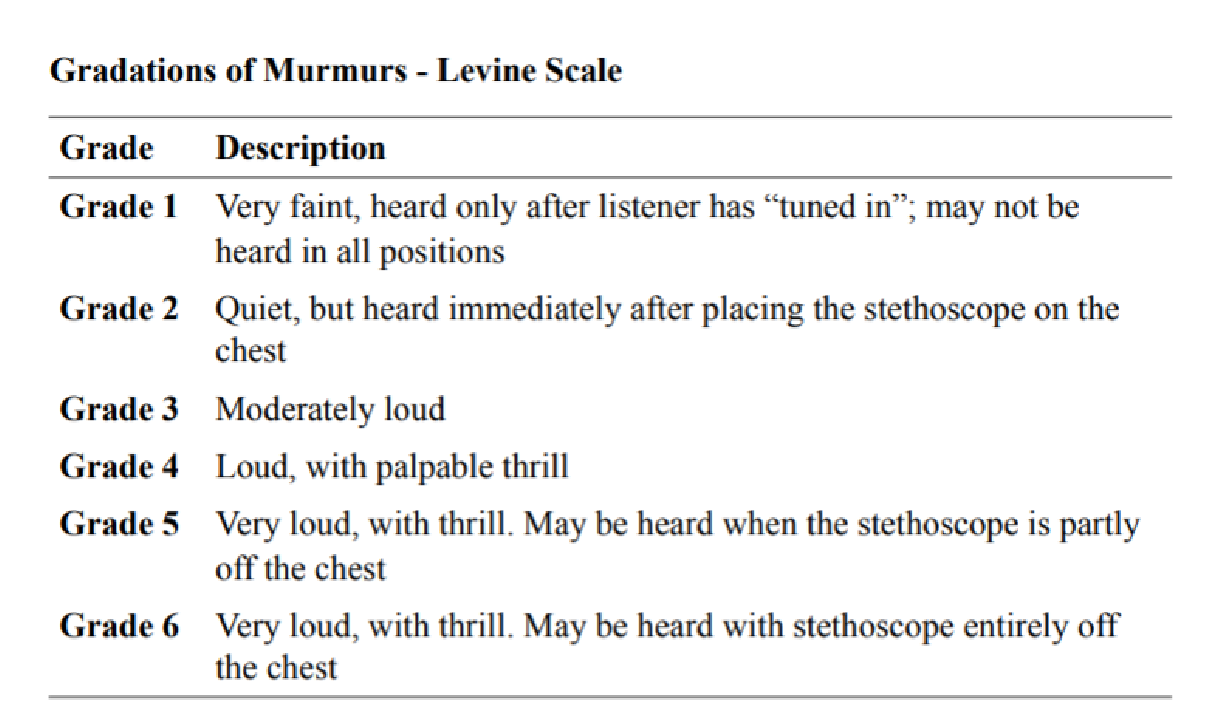 Data from palpation and auscultation– Data from palpation of radial artery, carotid, femoral, popliteal, tibial posterior, dorsal pedal pulsations-
Data from palpation and auscultation– Data from palpation of radial artery, carotid, femoral, popliteal, tibial posterior, dorsal pedal pulsations-
characteristics of
pulse waves. Bilateral
palpation of arteriescomparison of pulsation.
Data from the measurement of blood pressure.
– Abdomen – shape, size (circumference), participation in breathing, changes in the skin of the abdomen – scars, rashes, shunting, navel, visible peristalsis
Data on auscultation – motility and peristalsis
Data on percussion – ascites or tumor masses
Data from palpation – pain in the epigastric, in the course of the colon or in the umbilicus, increased liver (accurate dimensions in cm), enlarged spleen (size in centimeters).
Kidneys and urinary system – data sukusio renalis (painful or not, palpation kidney, palpation along the ureter and in the bladder. In men, if necessary, the prostate gland.
Limbs – length, volume position. Changes in joints – tenderness, swelling, redness, local temperature, locomotion-passive and active. Musculature – hypotrophy and tenderness.
Peripheral nervous system and tendon reflex
33. Nephrotic syndrome
•Proteinuria >3.5 g per 1.73 m2 per 24 h
•Hypoalbuminemia
•Edema
•Hyperlipidemia
•Casts
•Lipiduria
•It is characterized by massive proteinuria (>3.5g/m2/day), resultant hypoalbuminemia, induces hyperlipidemia and final edema which is generalized & also known as anasarca or dropsy. Puffiness around the eyes, especially in the morning, pale pitting edema over the legs, pleural effusion and ascites •Hyperlipidemia is caused by two factors:
1.Hypoproteinemia stimulates protein synthesis in the liver, resulting in the overproduction of lipoproteins.
2.Lipid catabolism is decreased due to lower levels of lipoprotein lipase, the main enzyme involved in lipoprotein breakdown Common underlying conditions:
•MCD – Minimal change disease
•FSGS- Focal segmental glomerulosclerosis
•MN- Membranous nephropathy
•MPGN- Membranoproliferative GN
•Diabetes
Inflammation and damage to the glomerulus result in damaged podocytes. The function of the podocytes is to prevent protein loss. When damaged proteins pass into the nephrotic tubule. Loss of antibodies (proteins) means they are at an increased risk of infection. Loss of protein from circulation results in hypoproteinemia- hypoalbuminemia.
The liver produces more proteins albumin and cholesterol- hypercholesterolemia. Hypoproteinemia results in reduced plasma oncotic pressure so water and electrolytes move into the interstitium from circulation resulting in peripheral edema. Decreased vascular volume results in decreased venous return to the heart, so less blood is pumped to the body, a decreased GFR initiates renin release. The RAAS system is activated through Na and water retention increases edema.
Dyslipidemia=xanthelasma and xanthomata (cholesterol deposits around eyes and hands), tiredness, periorbital, ascites or peripheral. Breathlessness due to pulmonary edema or pleural effusion. Frothy urine.
Investigations: urine dipstick, full blood count, liver function test, autoimmune screens. Chest X ray can show pleural effusion or edema. Ultrasound of kidney. Renal biopsy to check; light microscopy, immunofluorescence and electron microscopy.
Types of nephrotic syndrome
Primary nephrotic syndromes;
1- Minimal change disease
2-Membranous glomerulo-nephritis 3-Focal segmental glomerulosclerosis Secondary nephrotic syndrome:
1- Lupus
2-Diabetic nephropathy
3- Hepatitis B&C
4-Amyloidosis
34. Nephritic syndrome
Nephritic syndrome is the name given to a collection of different signs and symptoms that occur as a result of inflammation in the kidneys. This inflammation causes the kidneys to work less effectively. It also causes protein and red blood cells to leak from the bloodstream into the urine. Can be acute or chronic. Chronic inflammation of the kidneys can cause scarring, which may negatively impact kidney function and lead to high blood pressure and, eventually, if left undiagnosed and untreated, to a need for dialysis (renal replacement therapy, when a dialysis machine replaces the kidneys’ function and filters waste products from the blood), and possibly kidney transplantation.
Common causes are infections, immune system disorders and inflammation of the blood vessels. The main symptoms are passing less urine than normal, leading to a fluid buildup in the body, and having blood in the urine. People with nephritic syndrome also often develop high blood pressure. Nephritic syndrome is not a disease but a syndrome. A syndrome is a group of symptoms that often and predictably occur together, and which develop as a result of another condition. Syndromes are not necessarily specific to any disease or disorder.
CAUSES
Nephritic syndrome is the result of inflammation affecting small groups of blood vessels, known as glomeruli, in the kidneys. As the glomeruli are the kidneys’ main filter units, this inflammation disrupts the kidneys’ ability to adequately filter blood. The inflammation can originate in the kidneys themselves or be the result of infection or injury elsewhere in the body. It can occur in people of any age, including children.
It can develop as a result of the following:
- Primary glomerular diseases: Such as IgA nephropathy (Berger’s disease) or membranoproliferative glomerulonephritis. IgA nephropathy is a very common cause of nephritic syndrome.
- Bacterial infections: Such as MRSA, pneumococcal pneumonia, typhoid, infective endocarditis, or secondary syphilis. Nephritic syndrome following a streptococcal throat infection is fairly common, especially in children
- Viral infections: Such as HBV, mumps, measles, chickenpox or glandular fever (mononucleosis)
● Multisystem systemic/inflammatory diseases: Such as vasculitis, Goodpasture’s
Syndrome, granulomatosis with polyangiitis, Henoch-Schönlein purpura, or lupus (systemic lupus erythematosus)
- Abdominal abscess: A pocket of infected fluid and pus inside the abdominal cavity. This can be located on or near any organ
- Parasitic infections: Such as malaria.
SYMPTOMS
- Edema in the face and legs
- Oliguria
- Hematuria
- Proteinuria
- High blood pressure
- Fever, weakness and fatigue
- Appetite loss, vomiting and abdominal pain ● Malaise
DIAGNOSIS
○ Nephritic sediment
■ Hematuria (either micro- or intermittent macrohematuria)
■ Dysmorphic red blood cells (acanthocytes)
■ Red blood cell casts
■ Mild to moderate proteinuria of > 150 mg/24h but < 3.5 g/24h (nonselective glomerular proteinuria)
■ Sterile pyuria and sometimes WBC casts
| ● | Renal biopsy: sometimes indicated in patients with a nonspecific disease pattern to confirm diagnosis |
| ● | Blood tests |
○ V’Creatinine6’W’GFR
○ Azotemia’.*-/’V’X!@’
TREATMENT
| ● | Supportive therapy |
○ Low-sodium diet
○ Water restriction
| ● | Medical therapy |
○ If proteinuria and/or hypertension: angiotensin-converting enzyme inhibitors or angiotensin-receptor blockers
○ If severe hypertension and/or edema: diuretics ○ Sometimes immunosuppressive therapy is indicated.
| ● | If severe renal insufficiency or kidney failure: renal replacement therapy (e.g., hemodialysis, possibly transplantation) |
31. Acute renal failure.
YD#-(’0(,$%’C$*%#0(’EYZ[G’10’$D#-(’8*+,(&’*,\#0&’EY]^G6’*”’$”’$’=($”#0$>%(’*,D0($”(’*,’-/(’”(0#=’ D0($-*,*,(’EF0G’D1,D(,-0$-*1,’E#”#$%%&’0(%$-*)(’*,D0($”(’1C’4B5’10’$>”1%#-(’*,D0($”(’>&’__‘33’ a=1%NO’HB:4‘K:B’=MN+OIG6’1DD#0″’*,’b4‘75’1C’/1″?*-$%*c(+’?-“:’
- associated with increase in in-hospital mortality and morbidity.
- AKI can be anticipated in some clinical circumstances (e.g., after radiocontrast exposure or major surgery), and there are no specific pharmacologic therapies proven helpful at preventing or reversing the condition.
- AKI is a clinical diagnosis and not a structural one. A pt may have AKI with or without injury to the kidney parenchyma.
- AKI can range in severity from asymptomatic and transient changes in laboratory parameters of glomerular filtration rate (GFR), to overwhelming and rapidly fatal derangements in effective circulating volume regulation and electrolyte and acid-base composition of the plasma.
- Maintaining optimal renal perfusion and intravascular volume is critical in most clinical circumstances; important cofactors in AKI include hypovolemia and drugs that interfere with renal perfusion and/or glomerular filtration (nonsteroidal anti-inflammatory drugs [NSAIDs], angiotensin-converting enzyme [ACE] inhibitors, and angiotensin receptor blockers).
Differential diagnosis:
1. Prerenal failure
- most common among hospitalized pts.
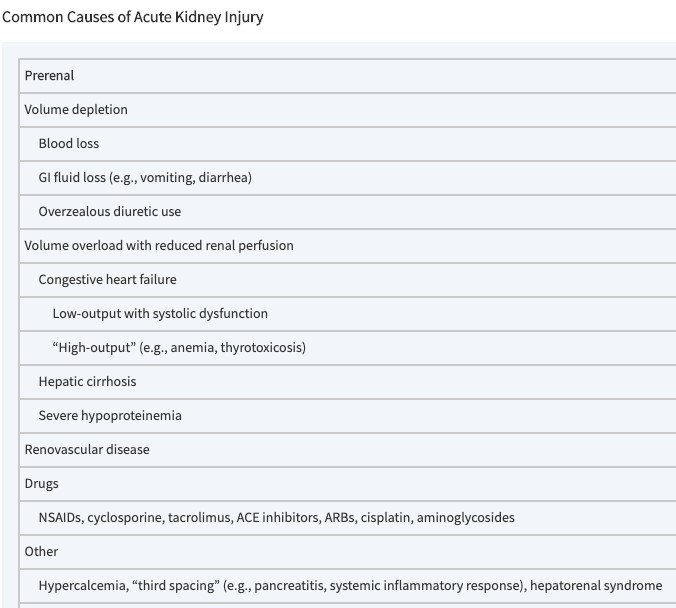 may result from true volume depletion (e.g., diarrhea, vomiting, GI or other hemorrhage) or “arterial underfilling,” i.e., reduced renal perfusion in the setting of adequate or excess blood volume. -> Reduced renal perfusion may be seen in congestive heart failure (CHF) (due to reduced cardiac output and/or potent vasodilator therapy), hepatic cirrhosis (due mostly to peripheral vasodilation and arteriovenous shunting), nephrotic syndrome and other states of severe hypoproteinemia (total serum protein <54 g/L [<5.4 g/dL]), and renovascular disease (because of fixed stenosis at the level of the main renal artery or large branch vessels).
may result from true volume depletion (e.g., diarrhea, vomiting, GI or other hemorrhage) or “arterial underfilling,” i.e., reduced renal perfusion in the setting of adequate or excess blood volume. -> Reduced renal perfusion may be seen in congestive heart failure (CHF) (due to reduced cardiac output and/or potent vasodilator therapy), hepatic cirrhosis (due mostly to peripheral vasodilation and arteriovenous shunting), nephrotic syndrome and other states of severe hypoproteinemia (total serum protein <54 g/L [<5.4 g/dL]), and renovascular disease (because of fixed stenosis at the level of the main renal artery or large branch vessels).- Several drugs can reduce renal perfusion, most notably NSAIDs. ACE inhibitors and angiotensin II receptor antagonists may reduce GFR but do not tend to reduce renal perfusion.
2. Intrinsic Renal Failure
- Causes depend on the clinical setting.
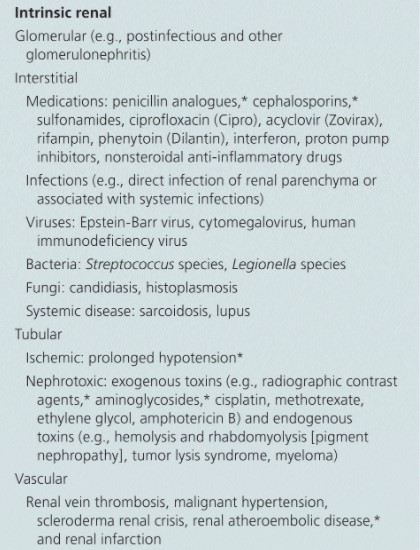 Among hospitalized pts, especially on surgical services/intensive care units, acute tubular necrosis (ATN) is the most common diagnosis.
Among hospitalized pts, especially on surgical services/intensive care units, acute tubular necrosis (ATN) is the most common diagnosis.- Ischemic events or toxic exposure (e.g., aminoglycoside therapy) may lead to in-hospital ATN.
- Or, pts may be admitted to the hospital with ATN associated with rhabdomyolysis; common predisposing factors in rhabdomyolysis include alcoholism, hypokalemia, and various drugs (e.g., statins).
- Allergic interstitial nephritis, usually due to antibiotics (e.g., penicillins, cephalosporins, sulfa drugs, quinolones, and rifampin), or NSAIDs, may also be responsible. More recently, the use of immune checkpoint inhibitors in cancer therapy has been linked to the development of interstitial nephritis.
- Radiographic contrast dyes may cause AKI in pts with pre existing kidney disease; risk is higher in diabetics with chronic kidney disease.
- Coronary angiography, other vascular procedures, thrombolysis, or anticoagulation may lead to atheroemboli, which cause AKI due to both hemodynamic and inflammatory effects; livedo reticularis, embolic phenomena with preserved peripheral pulses, and eosinophilia are important clues to this diagnosis.
- Acute glomerulonephritis (GN) and thrombotic microangiopathies may also cause AKI.
- Thrombotic microangiopathies can be clinically subdivided into renal-limited forms (e.g., Escherichia coli–associated hemolytic uremic syndrome [HUS]) and systemic forms (e.g., thrombotic thrombocytopenic purpura [TTP]).
- “Atypical HUS,” occurring in the absence of HUS-associated bacterial toxins, is associated with hereditary mutations in complement proteins or complement regulatory proteins, leading to exaggerated endothelial sensitivity to complement-mediated cytolysis.
- A variety of drugs can cause thrombotic microangiopathies, including calcineurin inhibitors (cyclosporine and tacrolimus), quinine, antiplatelet agents (e.g., ticlopidine), inhibitors of the action of vascular endothelial growth factor (VEGF), and chemotherapeutics (e.g., and gemcitabine).
- Important associated disorders in TTP include HIV infection, bone marrow transplantation, systemic lupus erythematosus (SLE), and antiphospholipid syndrome.
3. Postrenal failure
 is due to urinary tract obstruction – more common among ambulatory rather than hospitalized pts. More common in men than women,
is due to urinary tract obstruction – more common among ambulatory rather than hospitalized pts. More common in men than women,- It is most often caused by ureteral or urethral blockade.
- Occasionally, stones, sloughed renal papillae, or malignancy (primary or metastatic) may cause more proximal obstruction.
CHARACTERISTIC FINDINGS AND DIAGNOSTIC WORKUP
- All pts with AKI manifest some degree of azotemia (increased blood urea nitrogen [BUN] and Cr).
- Other clinical features depend on the etiology of renal disease.
- Pts with prerenal azotemia due to volume depletion usually demonstrate orthostatic hypotension, tachycardia, low jugular venous pressure, and dry mucous membranes.
- Pts with prerenal azotemia and CHF (“cardiorenal syndrome”) may show jugular venous distention, an S3 gallop, and peripheral and pulmonary edema.
- Therefore, the physical examination is critical in the workup of pts with prerenal AKI.
- In general, the BUN/Cr ratio is high (>20:1), more so with volume depletion and CHF than with cirrhosis.
- The uric acid may also be disproportionately elevated in noncirrhotic prerenal states (due to increased proximal tubular absorption).
- Urine chemistries tend to show low urine [Na+] (<10–20 mmol/L, <10 with hepatorenal syndrome) and a fractional excretion of sodium (FENa) of <1%.
- The urinalysis (UA) typically shows hyaline and a few granular casts, without cells or cellular casts. Renal ultrasonography is usually normal.
Pts with intrinsic renal disease present with varying complaints.
- GN is accompanied by hypertension and mild – moderate edema (associated with Na retention and proteinuria, and sometimes with gross hematuria).
- An antecedent prodromal illness and/or prominent extrarenal symptoms and signs may occur if GN occurs in the context of a systemic illness, e.g., vasculitis or SLE; these may be hemoptysis or pulmonary hemorrhage (vasculitis and Goodpasture’s syndrome), arthralgias/arthritis (vasculitis or SLE), serositis (SLE), and unexplained sinusitis (vasculitis).
- urine chemistries may be indistinguishable from those prerenal failure; some pts with GN have renal hypoperfusion (due to glomerular inflammation and ischemia) with resultant hyperreninemia leading to acute volume expansion and hypertension. The urine sediment can be very helpful in these cases.
- Red blood cells (RBC), white blood cells (WBC), and cellular casts are characteristic of GN; RBC casts are rarely seen in other conditions (i.e., they are highly specific).
- In the setting of inflammatory nephritis (GN or interstitial nephritis, see next), there may be increased renal echogenicity on ultrasonography.
- Unlike pts with GN, pts with interstitial diseases are less likely to have hypertension or proteinuria; exception is NSAID-associated acute interstitial nephritis, which is accompanied by proteinuria due to associated minimal-change glomerular lesion.
- Hematuria and pyuria may present on UA.
- Sediment finding in allergic interstitial nephritis is a predominance (>10%) of urinary eosinophils with Wright’s or Hansel’s stain; however, urinary eosinophils can be increased in several other causes of AKI, such that measurement of urine eosinophils has no diagnostic utility in renal disease.
- WBC casts may also be seen, particularly in cases of pyelonephritis.
- The urinary sediment of pts with ischemic or toxic ATN will characteristically contain pigmented “muddy-brown” granular casts and casts containing tubular epithelial cells; free tubular epithelial cells can also be seen.
- The FENa is typically >1% in ATN, but may be <1% in pts with milder, nonoliguric ATN (e.g., from rhabdomyolysis) and in pts with severe underlying “prerenal” disorders, such as CHF or cirrhosis.
Pts with postrenal AKI
- due to urinary tract obstruction are usually less severely ill than pts with prerenal or intrinsic renal disease, presentation may be delayed until azotemia is markedly advanced (BUN >54 µmol/L [150 mg/dL], Cr >1060–1325 µmol/L [12–15 mg/dL]).
- An associated impairment of urinary concentrating ability “protects” the pt from complications of volume overload.
- Urinary electrolytes typically show an FENa >1%, and microscopic examination of the urinary sediment is usually bland.
- Ultrasonography is the key initial diagnostic tool. More than 90% of pts with postrenal AKI show obstruction of the urinary collection system on ultrasound (e.g., dilated ureter, calyces); false negatives include hyperacute obstruction and encasement of the ureter and/or kidney by tumor or of the ureter by retroperitoneal fibrosis, functionally obstructing urinary outflow without structural dilation.
- Other imaging techniques, such as a furosemide renogram (MAG3 nuclear medicine study), may be required to define better the presence or absence of obstructive uropathy.
TREATMENT
= Etiology-specific supportive care.
1. Prerenal
- pts with prerenal failure due to GI fluid loss may experience relatively rapid correction of AKI after the administration of IV fluid to expand volume.
- The same treatment in prerenal pts with CHF would be counterproductive; in this case, treatment of the underlying disease with vasodilators and/or inotropic agents would more likely be of benefit.
2. Internal
- There are relatively few intrinsic renal causes of AKI for which there is safe and effective therapy.
- GN associated with vasculitis or SLE – high-dose glucocorticoids and cytotoxic agents (e.g., cyclophosphamide), or high-dose glucocorticoids and monoclonal antibodies against the CD20 protein on B cells (rituximab and related agents); plasmapheresis and plasma exchange may be useful in other selected circumstances (e.g., Goodpasture’s syndrome and TTP, respectively).
- Antibiotic therapy may be sufficient for the treatment of AKI associated with pyelonephritis or endocarditis. There are conflicting data regarding the utility of glucocorticoids in allergic interstitial nephritis. However, many practitioners advocate the use of glucocorticoids in pts with clinical evidence of progressive renal insufficiency despite discontinuation of the offending drug, or with biopsy evidence of potentially reversible, severe disease.
3. Postrenal
- The treatment of urinary tract obstruction often involves consultation with a urologist.
- Interventions as simple as Foley catheter placement or as complicated as multiple ureteral stents and/or nephrostomy tubes may be required.
32. Chronic renal failure
Chronic kidney disease (CKD) can be defined by the presence of kidney damage or reduced kidney function for three or more months. Reduced kidney function is suggested by a reduction in the glomerular filtration rate (GFR).
Kidney damage can be characterised by the presence of one of more of the following pathological markers.
- Albuminuria (e.g. albumin:creatinine ratio > 3 mg/mmol or > 30 mg/g)
- Urinary sediment abnormalities (e.g. white cell or red cell casts)
- Radiological abnormalities (e.g. polycystic kidneys) 4. Pathological abnormalities (e.g. seen on renal biopsy)
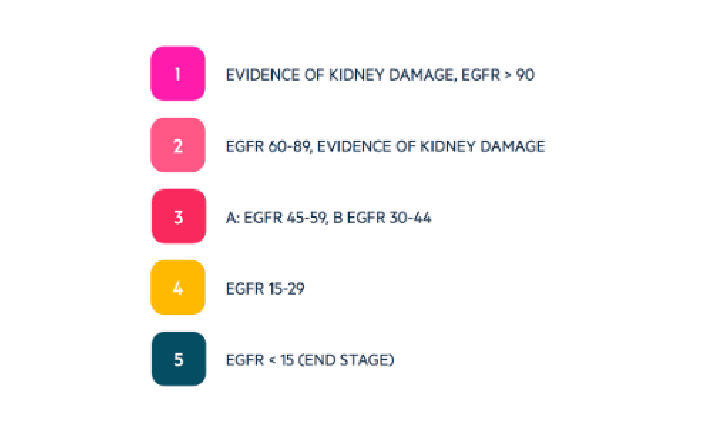
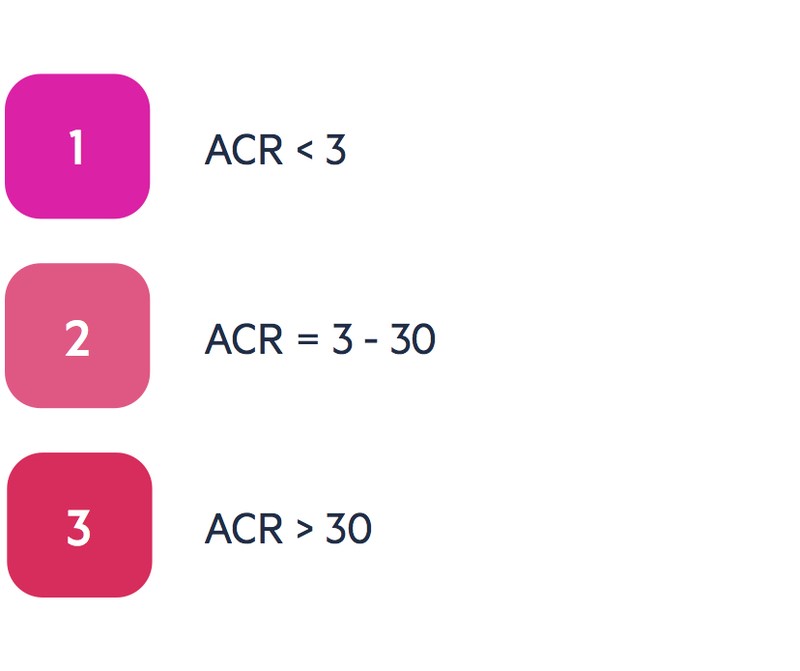
5. History of kidney transplantation.
CKD is a common condition with a progressive nature. As CKD progresses towards end-stage renal disease (ESRD) it is associated with more symptoms, increasing complications and need for renal replacement therapy (RRT). The inability of the kidneys to carry out their normal function can lead to problems with volume regulation, acid-base balance, calcium and phosphate handling and electrolyte abnormalities.
Classification
The classification of CKD is now based on two factors: the estimated glomerular filtration rate (eGFR, ml/min/1.73m2) and the albumin:creatinine ratio (ACR, mg/mmol). The change towards using ACR in the classification of CKD reflects the increased risk of acute on chronic injury, end stage disease and all-cause mortality in patients with a high ACR.
CKD is increasingly common with advancing age and stages 3-5 affect up to 8.5% of the adult population. The higher the stage of CKD, the more frequent monitoring patients require. This helps to identify and manage complications and plan for renal replacement therapy.
Major causes include:
- Hypertensive nephropathy
- Diabetic nephropathy
- Glomerulopathies
- Inherited kidney disorders (e.g. PCKD)
- Ischaemic nephropathy (e.g. vascular disease)
- Obstructive uropathy
- Tubulointerstitial diseases
- Medications
Approximately 1 million nephrons are present in each kidney from birth. These nephrons contribute to the kidneys ability to maintain adequate glomerular filtration and allow the kidney to perform its normal functions (e.g. volume regulation, acid-base balance). As we age there is a progressive loss in renal mass and a number of structural changes occur (e.g. glomerulosclerosis) leading to a decline in renal function. Following a peak in the third decade of life, there is an estimated annual decline of 1 mL/min/year in eGFR.
Regardless of the underlying cause, renal disease leads to progressive loss of nephrons and a subsequent reduction in the GFR. As the disease progresses, structural abnormalities may occur leading to kidney damage (e.g. albuminuria), and eventually, the kidneys start to lose their ability to carry out normal functions
Diagnosis
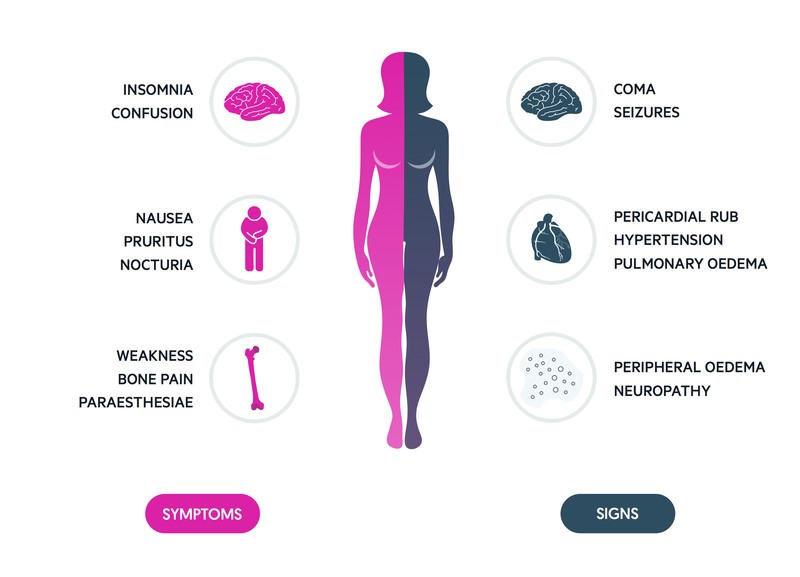 The diagnosis and subsequent monitoring of CKD is based on evidence of kidney damage and the measurement of the serum creatinine and urinary ACR.
The diagnosis and subsequent monitoring of CKD is based on evidence of kidney damage and the measurement of the serum creatinine and urinary ACR.
There are a number of ways to calculate the eGFR from serum creatinine, all should be used with caution. Serum creatinine levels have a high individual variation changing with disease states, muscle mass, pregnancy and dietary intake. Many laboratories will use the Modification of Diet in Renal Disease (MDRD) equation; however,
NICE recommend the use the
Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation for calculating the eGFR.
Indications for CKD testing include the following:
- Diabetes
- Hypertension
- Acute kidney injury
- Obesity with metabolic syndrome
- Cardiovascular disease
- Structural renal tract disease
- Proteinuria or persistent haematuria
- Family history
Depending on the results of the eGFR and ACR, patients can be classified into a particular stage of CKD. In patients with stable CKD (e.g. eGFR < 60ml/min without acute deterioration or ACR between 3 and 70 mg/mmol), it is important to repeat these tests within 3 months. Those with pronounced albuminuria (> 70mg/mmol) or significantly reduced eGFR (G4 or G5) require referral to a nephrologist.
Those with evidence of persistent haematuria in the absence of infection should be investigated for malignancy.
Management
The principles of CKD management are to treat the underlying cause, prevent or slow progression (e.g. renoprotective therapy), treat associated complications and plan for RRT.

Renal replacement therapy
Haemodialysis, peritoneal dialysis and renal transplant are all forms of RRT that are indicated for ESRD.
35. Urine analysis- proteinuria, haematuria, pyuria, tests of urine dilution and concentration.
Inspect urine
- Wash hands, use gloves and apron
- Confirm patient details are correct on the sample bottle – name / DOB / hospital number
- Inspect the colour of the urine:
- Straw coloured – normal
- Dark concentrated urine – dehydration
- Red – macroscopic haematuria / rifampicin / porphyria / beetroot
- Brown – bile pigments / myoglobin / antimalarials
- Inspect the clarity of the urine:
- Clear – normal
- Cloudy / debris – urinary tract infection (UTI)
- Frothy – nephrotic syndrome
- Remove the sample bottles’ cap and assess urine odour:
- Offensive urine – UTI
- Sweet – glycosuria
- Ketones – like nail polish remover – diabetes
Dipstick testing
- Check urine dipsticks’ expiry date
- Remove a testing strip from the container (avoiding touching the testing zones)
- Insert test strip into urine sample (ensuring all test zones are immersed)
- Remove the strip, ensuring to tap off residual urine before removing from the sample bottle 5. Ensure test strip remains in a horizontal orientation (to avoid cross contamination of testing zones)
- Use the dipstick analysis guide on the side of the testing strip container to interpret the findings
- Different tests on the strip are required to be read at different times, so ensure you interpret the appropriate test at the correct time interval – e.g. 60 seconds for protein
- Once you have interpreted all of the tests, discard the strip into the clinical waste bin along with your gloves and apron
- Wash hands
Indicators of Dipstick testing:
- ?S’‘’*,+*D$-(“’$D*+*-&’1C’#0*,(’‘’(:M:’W?S’*,’”&”-(=*D’$D*+1″*”
- R?(D*C*D’M0$)*-&’‘’*,+*D$-(“’$=1#,-’1C’”1%#-(’+*””1%)(+’*,’#0*,(’‘’W’*,’+*$>(-(“’*,”*?*+#”
- X%11+’’‘’*,+*D$-(“’,#=>(0’1C’0(+’>%11+’D(%%”’*,’#0*,(’‘’V’*,’/$(=$-#0*$
- d01-(*,’‘’*,+*D$-(“’%()(%’1C’?01-(*,’*,’-/(’#0*,(’‘’V’nephrotic syndrome
- O(#81D&-(’(“-(0$”(’‘’(,c&=(’?01+#D(+’>&’,(#-01?/*%”’EeFF’*,’#0*,(G’‘’V’*,’!f^ ● Nitrites – breakdown products caused by Gram -ve organisms – Gram -ve UTI e.g. Ecoli
- ](-1,(“’‘’>0($8+1.,’?01+#D-’1C’C$–&’$D*+’=(-$>1%*”=’‘’V’”-$0)$-*1,’N’Vg]Y
- h%#D1″(’‘’V’/&?(0M%&D$(=*$’(:M:’?110%&’D1,-01%%(+’+*$>(-(“
- X*%*0#>*,’‘’^,+*D$-(“’V’D1,\#M$-(+’>*%*0#>*,’E.$-(0’”1%#>%(G’‘’V’>*%*$0&’-0$D-’1>”-0#D-*1,
- !01>*%*,1M(,’‘’*C’0$*”(+’*,+*D$-(“’V’>*%*0#>*,’-#0,1)(0’‘’V=$%$0*$’N’V/$(=1%&-*D’$,$(=*$’
Further investigations may be required:
- V’eFF’N’O(#81D&-(“’‘’i!f^’‘’’”(,+’#0*,(’C10’D#%-#0(’EjR!NFR!G
- V’h%#D1″(’‘’ig*$>(-(“’‘’’D$?*%%$0&’>%11+’M%#D1″(
| Abnormal urine dipstick findings | |
| Proteinuria |
|
| Haematuria |
|
| Glycosuria |
|
| Ketones | Diabetic ketoacidosis, pregnancy, after starvation and dehydration (often present in gastroenteritis / dehydration), rapid weight loss |
| Bilirubin and urobilogen | ● Normal urine contains no bilirubin, and very little urobilogen Conjugated bilirubin may appear in the urine in the presence of liver disease, or bile duct obstruction. |
| Leukocytes | ●This test has lower specificity for infection than nitrites, and thus testing for nitrites is seen as for the presence of infection. ●Be wary of diagnosing a UTI based of leukocytes only. In my practice (as a GP) in a well, asymptomatic patient I will often send these samples for MC+S without treating, to confirm if a UTI is present. ●However, especially in the elderly, leucocytes only may indicate a UTI |
| pH | ●Should be between 4.5 and 5.3 ●A metabolic acidosis and alkaloid urine suggests a renal tubular acidosis. These patients have a risk of stone formation and nephrocalcinosis ●Acidic urine can be caused by diet and uric acid calculi ●Note that stale urine can become alkaline – thus you should check if the urine has been left for any period of time |
| Nitrites | ●The presence of nitrites is essentially diagnostic for UTI |
| ●Nitrites are produced by bacteria; and thus raised levels indicate the presence of bacteria in the urine. Accuracy may be affected in symptomatic patients, and patients on antibiotics. ○ Urine should usually be sterile ○ Patients with catheters often have | |
| Pyuria | ●Is the condition of urine containing white blood cells or pus. ●Presence of 6-10 or more neutrophils per high power field of unspun, voided mid-stream urine, it can be a sign of a bacterial urinary tract infection. ●Pyuria may be present in the people with sepsis, or in older people with pneumonia. |
| Specific gravity | ●shows concentration of solutes in the urine; and is thus a measure of the ability of the kidneys to concentrate fluids. ●If the value is high: ○ Dehydration ○ Glycosuria ○ Proteinuria ○ Renal artery stenosis ●If the value is low ○ Excess fluid intake ○ Renal failure ○ Pyelonephritis ○ Diabetes insipidus |
| Abnormal urine dipstick findings | |
| Proteinuria | Healthy adults excrete 80-120mg protein / day. Up to 1g per day, usually at night – too small to be detected on dipstick testing. The dipstick can detect 20-30mg / dl. Proteinuria may indicate; renovascular, glomerular or tubulointerstitial renal disease, or a sign of diseases that cause overproduction of urine, such as myeloma. False negatives can occur with very diluted urine and/or when the primary protein is not albumin. Also occur in very alkaline conditions. Transient proteinuria – in young patients it’s usually not a problem, and resolves within a few days, or after >8 hours lying down. In older patients it may be a sign of congestive heart failure. Intermittent proteinuria – present in young adults as a result of prolonged vertical posture, exposure to cold, pregnancy and hypertension. This usually produces about 1g of protein per day. This is asymptomatic, and should only ever be treated in renal problems. Persistent – due to underlying disease, most commonly; glomerular. This often produces in excess of 2g protein per day. Can also be due to overflow proteinuria (myeloma), connective tissue disorders, DM, hypertension. Pre-eclampsia – a condition in pregnant women characterised by hypertension and proteinuria. |
| Haematuria | F1,-$=*,$-*1,’C01=’=(,”-0#$%’>%((+*,M’k’=1″-’D1==1,’D$#”( Recent trauma Prostate examination Other recent urological examination (e.g. cystoscopy) Glomerular or tubular pathology Urologic pathology – this present with haematuria without proteinuria Exercise induced – long distance runner. Result will be negative if repeated after 72 hours with no further exercise Dehydration Urine dipstick test is 90% sensitive, but less specific. However, only 0.5-6% of patients have significant underlying pathology |
| Glycosuria | Small amounts of urine are naturally excreted. The actual amount varies with the renal threshold from patient to patient. Generally these levels are too small to be detected on urine dipstick. Can be caused by diabetes, Cushing’s syndrome, liver and pancreatic disease, Fanconi’s syndrome |
| Ketones | Diabetic ketoacidosis, pregnancy, after starvation and dehydration (often present in gastroenteritis / dehydration), rapid weight loss |
| Bilirubin and urobilogen | ●Normal urine contains no bilirubin, and very little urobilogen Conjugated bilirubin may appear in the urine in the presence of liver disease, or bile duct obstruction. |
| Leukocytes | ●This test has lower specificity for infection than nitrites, and thus testing for nitrites is seen as for the presence of infection. |
| ●Be wary of diagnosing a UTI based of leukocytes only. In my practice (as a GP) in a well, asymptomatic patient I will often send these samples for MC+S without treating, to confirm if a UTI is present. | |
| ●However, especially in the elderly, leucocytes only may indicate a UTI | |
| pH | ●Should be between 4.5 and 5.3 |
| ●A metabolic acidosis and alkaloid urine suggests a renal tubular acidosis. These patients have a risk of stone formation and nephrocalcinosis | |
| ●Acidic urine can be caused by diet and uric acid calculi | |
| ●Note that stale urine can become alkaline – thus you should check if the urine has been left for any period of time | |
| Nitrites | ●The presence of nitrites is essentially diagnostic for UTI |
| ●Nitrites are produced by bacteria; and thus raised levels indicate the presence of bacteria in the urine. Accuracy may be affected in symptomatic patients, and patients on antibiotics. | |
| ○Urine should usually be sterile | |
| ○Patients with catheters often have | |
| Pyuria | ●is the condition of urine containing white blood cells or pus. |
| ●presence of 6-10 or more neutrophils per high power field of unspun, voided mid-stream urine, it can be a sign of a bacterial urinary tract infection. | |
| ●Pyuria may be present in the people with sepsis, or in older people with pneumonia. | |
| Specific gravity | ●shows concentration of solutes in the urine; and is thus a measure of the ability of the kidneys to concentrate fluids. |
| ●If the value is high: | |
| ○Dehydration | |
| ○Glycosuria | |
| ○Proteinuria | |
| ○Renal artery stenosis | |
| ●If the value is low | |
| ○Excess fluid intake | |
| ○Renal failure | |
| ○Pyelonephritis | |
| ○Diabetes insipidus |
36. Renal function examination
Assessment of renal function is important in the management of patients with kidney disease or pathologies affecting renal function. Tests of renal function have utility in identifying the presence of renal disease, monitoring the response of kidneys to treatment, and determining the progression of renal disease.
Assessment of Renal Function
There are a number of clinical laboratory tests that are useful in investigating and evaluating kidney function. Clinically, the most practical tests to assess renal function is to get an estimate of the glomerular filtration rate (GFR) and to check for proteinuria (albuminuria).
Glomerular Filtration Rate
The best overall indicator of the glomerular function is the glomerular filtration rate (GFR). The normal GFR for an adult male is 90 to 120 mL per minute. GFR is the rate in milliliters per minutes at which substances in plasma are filtered through the glomerulus, in other words, the clearance of a substance from the blood. The characteristics of an ideal marker of GFR are as follows:
- It should appear endogenously in the plasma at a constant rate
- It should be freely filtered at the glomerulus
- It can be neither reabsorbed nor secreted by the renal tubule ● It should not undergo extrarenal elimination.
As no such endogenous marker currently exists, exogenous markers of GFR are used. Assessment of GFR using inulin, a polysaccharide, is considered the reference method for assessment of GFR. It involves the infusion of inulin and then measurement of blood levels after a specified period to determine the rate of clearance of inulin. Other exogenous markers used are radioisotopes such as chromium-51 ethylene-diamine-tetra-acetic acid (51 Cr-EDTA), and technetium-99-labeled diethylene-triamine-pentaacetate (99 Tc-DTPA). The most promising exogenous marker is the non-radioactive contrast agent, iohexol, especially in children.
The inconvenience associated with the use of exogenous markers, specifically that testing has to be performed in specialized centers, and the difficulty to assay these substances, has encouraged the use of endogenous markers.
Creatinine
The most commonly used endogenous marker for assessment of glomerular function is creatinine. The calculated clearance of creatinine is used to provide an indicator of GFR. This involves the collection of urine over a 24-hour period or preferably over an accurately timed period of 5 to 8 hours since 24-hour collections are notoriously unreliable. Creatinine clearance is then calculated using the equation:
C = (U x V) / P
C = clearance, U = urinary concentration, V = urinary flow rate (volume/time ie ml/min), and P = plasma concentration
Creatinine clearance should be corrected for body surface area. Improper or incomplete urine collection is one of the major issues affecting the accuracy of this test, hence timed collection is advantageous. Furthermore, due to tubular secretion, creatinine overestimates GFR by around 10% to 20%.
Serum creatinine is also utilized in GFR estimating equations such as the Modified Diet in Renal Disease (MDRD) and the CKD-EPI equation. These eGFR equations are superior to serum creatinine alone since they include race, age, and gender variables. GFR is classified into the following stages based on the kidney disease.
Improving Global Outcomes (KDIGO) stages of chronic kidney disease (CKD):
- Stage 1 GFR greater than 90 ml/min/1.73 m
- Stage 2 GFR-between 60 to 89 ml/min/1.73 m
- Stage 3a GFR 45 to 59 ml/min/1.73 m
- Stage 3b GFR 30 to 44 ml/min/1.73 m
- Stage 4 GFR of 15 to 29 ml/min/1.73 m
- Stage 5-GFR less than 15 ml/min/1.73 m (end-stage renal disease)
These provide an easier estimation of GFR without collection of urine or use of exogenous materials. However, as they utilize serum creatinine, they are also affected by the issues around serum creatinine measurement, hence the correction for race, gender, and age.
Blood Urea Nitrogen (BUN)
Urea or BUN is a nitrogen-containing compound formed in the liver as the end product or protein metabolism and urea cycle. About 85% of urea is eliminated via kidneys; the rest is excreted via the gastrointestinal (GI) tract. Serum urea is increased in conditions where renal clearance decreased (in acute and chronic renal failure/impairment). Urea may also increase in other conditions not related to renal diseases such as upper GI bleeding, dehydration, catabolic states, and high protein diets. Urea may be decreased in starvation, low-protein diet, and severe liver disease. Serum creatinine is a more accurate assessment of renal function than urea; however, urea is increased earlier in renal disease.
Kidney function tests usually require a 24-hour urine sample and a blood test. A 24-hour urine sample is a creatinine clearance test. It gives your doctor an idea of how much creatinine your body expels over a single day. BUN and serum creatinine tests require blood samples taken in a lab or doctor’s office.
37. X-ray, isotopic and other imaging methods of examination of the urinary tract system
X-RAY
Kidney, Ureter, and Bladder (KUB) X–ray
- A kidney, ureter, and bladder (KUB) X-ray may be performed to assess the abdominal area for causes of abdominal pain, or to assess the organs and structures of the urinary and/or gastrointestinal (GI) system
- A KUB X-ray may be the first diagnostic procedure used to assess the urinary system. – X-rays use invisible electromagnetic energy beams to produce images of internal tissues, bones, and organs on film. X-rays are made by using external radiation to produce images of the body, its organs, and other internal structures for diagnostic purposes. X-rays pass through body tissues onto specially treated plates (similar to camera film) and a “negative” type picture is made (the more solid a structure is, the whiter it appears on the film). Digital films and digital media are more commonly used now than the film media.
Computed tomography (CT scan or CAT scan)
- is a noninvasive diagnostic imaging procedure that uses a combination of X-rays and computer technology to produce horizontal, or axial, images (often called slices) of the body. – A CT scan shows detailed images of any part of the body, including the bones, muscles, fat, and organs. CT scans are more detailed than standard X-rays. – CT scans of the kidneys can provide more detailed information about the kidneys than standard kidney, ureter, and bladder (KUB) X-rays , thus providing more information related to injuries and/or diseases of the kidneys.
- CT scans of the kidneys are useful in the examination of one or both of the kidneys to detect conditions such as tumors or other lesions, obstructive conditions, such as kidney stones, congenital anomalies, polycystic kidney disease, accumulation of fluid around the kidneys, and the location of abscesses.
Ultrasound of the Kidney
-A kidney ultrasound is a noninvasive diagnostic exam that produces images, which are used to assess the size, shape, and location of the kidneys. Ultrasound may also be used to assess blood flow to the kidneys.
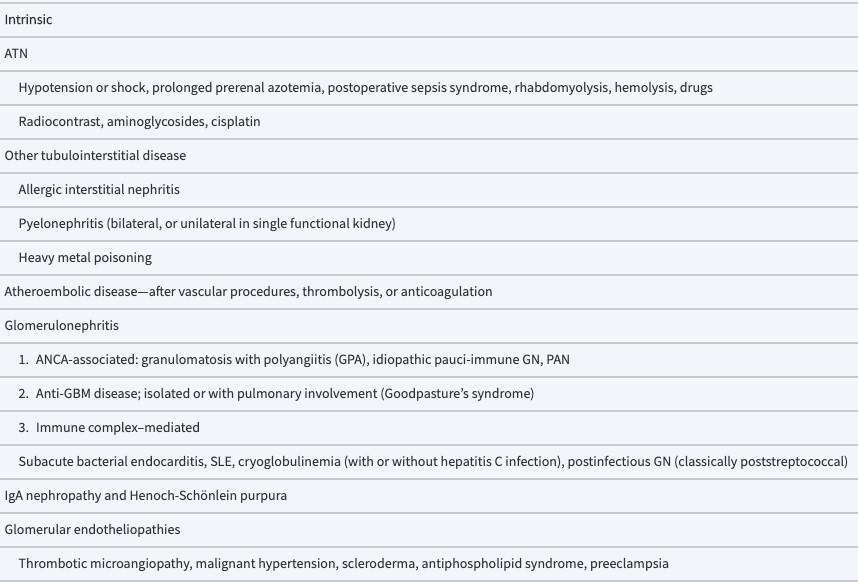 -Ultrasound uses a transducer that sends out ultrasound waves at a frequency too high to be heard. The ultrasound transducer is placed on the skin, and the ultrasound waves move through the body to the organs and structures within. The sound waves bounce off the organs like an echo and return to the transducer. The transducer processes the reflected waves, which are then converted by a computer into an image of the organs or tissues being examined.
-Ultrasound uses a transducer that sends out ultrasound waves at a frequency too high to be heard. The ultrasound transducer is placed on the skin, and the ultrasound waves move through the body to the organs and structures within. The sound waves bounce off the organs like an echo and return to the transducer. The transducer processes the reflected waves, which are then converted by a computer into an image of the organs or tissues being examined.
-The sound waves travel at different speeds depending on the type of tissue encountered – fastest through bone tissue and slowest through air. The speed at which the sound waves are returned to the transducer, as well as how much of the sound wave returns, is translated by the transducer as different types of tissue. – An ultrasound gel is placed on the transducer and the skin to allow for smooth movement of the transducer over the skin and to eliminate air between the skin and the transducer for the best sound conduction
Renal osteodystrophy
-Renal osteodystrophy is currently defined as an alteration of bone morphology in patient with chronic kidney disease (CKD).
-It is one measure of the skeletal component of the systemic disorder of chronic kidney disease-mineral and bone disorder (CKD-MBD)
Renal Angiogram
- A renal angiogram is an imaging test to look at the blood vessels in your kidneys. Your healthcare provider can use it to look at the ballooning of a blood vessel (aneurysm), narrowing of a blood vessel (stenosis), or blockages in a blood vessel. He or she can also see how well blood is flowing to your kidneys.
- For the test, the radiologist injects a contrast dye into the artery that brings blood into the kidney. Then he or she uses X-ray images to watch the dye as it flows through the blood vessels in the kidneys.
- X-rays use a small amount of radiation to create images of your bones and internal organs. A renal angiogram is one type of X-ray.
Artificial Kidney. Chronic Hemodialysis
- artificial kidneys (hemodialyzer) are used to remove waste and extra chemicals and fluid from your blood. To get your blood into the artificial kidney, the doctor needs to make an access (entrance) into your blood vessels.
- This is done by minor surgery to your arm or leg.
- Sometimes, an access is made by joining an artery to a vein under your skin to make a bigger blood vessel called a fistula.
Intravenous pyelogram
- An IVP is an imaging test used to look at the kidneys and ureters. The ureters are the narrow tubes that carry urine from the kidneys to the bladder.
-During the test, the radiologist injects a contrast dye into one of your veins. He or she uses X-ray images to watch the contrast dye as it moves from the kidney into the ureter and then to the Bladder.
- Dye that moves too slowly or not at all may mean that you have a blockage in the blood flow through a kidney. It may also mean that the kidney, ureter, or bladder is not working as well as it should.
Renal osteodystrophy Hemodialysis Renovasography

38. Physical examination of the abdomen. Ascites
History – critical element in the evaluation
Mode of onset, progression, character, and severity of pain
- Pain that is sudden in onset, severe or explosive, progressive, continuous, and lasts more than 6 hours generally indicates surgical etiology.
- Pain that is gradual in onset, mild to moderate in intensity, intermittent, recurrent, or resolves partially or completely in less than 6 hours favors a nonsurgical diagnosis.
- Pain arising in a hollow, tubular structure, such as the ureter, intestine, biliary radicles, or fallopian tubes, may be continuous or intermittent. The severity of such pain is inversely proportional to the diameter of the tubular structure involved.
Initial location of pain
- In general, the farther from the umbilicus the pain localizes, the greater the chance that a surgical condition exists.
- Pain arising from foregut derivatives (stomach, duodenum, biliary tract, and pancreas) or the spleen presents in the epigastrium.
- Pain arising from midgut derivatives (jejunum, ileum, proximal third of the colon, and appendix) presents in the periumbilical area.
- Pain arising from the embryonic hindgut (distal two-thirds of the colon), internal reproductive organs (ovaries, fallopian tubes, uterus, seminal vesicles, and prostate), and the urinary bladder presents in the hypogastrium.
Any shift of pain
- A shift in pain occurs when the original inflammation extends to the parietal peritoneum.
- For example, appendicitis initially causes pain in the periumbilical area. Then, after 4 to 6 hours, the inflammation extends to the regional peritoneal surface and is perceived in the right lower quadrant
Associated symptoms and their temporal relationship to the pain
- Vomiting, nausea and anorexia
- In surgical conditions, pain may be followed by nausea, vomiting, and anorexia.
- In nonsurgical conditions nausea, vomiting, and anorexia typically precede pain.
- Additionally, clinical experience has shown that vomiting in the obese patient is an ominous symptom and virtually always suggests serious abnormalities.
- Fever is a common finding in patients who have abdominal pain; however, fever and chills is rarely seen in surgical processes. This combination suggests infection in the urinary tract, respiratory system, etc.
- Constipation may accompany any abdominal condition that causes an illness. Obstipation—non passage of both stool and gas—however, always suggests a surgical problem.
- Diarrhea, especially with cramps, indicates gastroenteritis and other nonsurgical conditions like inflammatory bowel disease
What aggravates the pain
- Always ask first about which activities aggravate the pain. (One can generally assume that the opposite will ease the pain.) If the patient hears questions about what eases the pain, he or she may perceive it as minimizing the problem and become defensive.
- Coughing, sneezing, rapid movements, and walking, especially down stairs, can cause peritoneal irritation.
- Musculoskeletal pain is often relieved by changing position.
- A bowel movement often eases the pain of gastroenteritis, but the pain may promptly recur.
Menstrual history and reproductive status
- Among sexually active people, women experience abdominal pain twice as often as men of the same age. Men who do experience abdominal pain, however, have a higher incidence of surgical disease. This disparity is generally because of the painful conditions affecting the female genitourinary tracts—nonsurgical (pelvic inflammatory disease, endometriosis, dysmenorrhea, and urinary tract infection) and surgical (torsion
of ovary and ectopic pregnancy). In men, seminal vesiculitis, prostatitis, and urethritis can cause lower abdominal pain.
- Pain that is severe, sudden in onset, and follows an abnormal menstrual period might stem from an ectopic pregnancy.
- Pain that is noted shortly after a normal menstrual period, is bilateral, and is accompanied by a fever and abdominal pain—but not nausea and vomiting—favors pelvic inflammatory disease.
Medications and supplements
- Aspirin and other nonsteroidal anti-inflammatory drugs, erythromycin, potassium, and salt tablets commonly cause gastric irritation and abdominal pain.
- Previous episodes, family history of similar problems, peers with the same symptoms, food intolerance, allergies, sudden changes in diet, and travel to regions with endemic disease
- These all favor a nonsurgical diagnosis.
Physical examination
Some keys to the physical exam:
- Before beginning, tell the patient what will transpire—and why. Assure the patient that any test that causes pain or discomfort will be discontinued.
- Auscultation should precede other modalities that involve physical contact. This will prevent alteration of peristalsis by physical stimulation.
- All portions of the exam that involve contact with the abdomen (auscultation, light touch, palpation, and percussion) should begin in the area farthest from the site of maximal pain
- steps that involve physical contact should be done with the patient relaxing the muscles as much as possible. Then repeat with the patient tensing the abdominal muscles (voluntary guarding). If the pain from a given maneuver increases with guarding, the source of the pain is in the abdominal wall. If pain is lessened by guarding, the source is visceral.
- If the patient seems to be overreacting to palpation, or if guarding does not seem genuine, ask the patient questions and have him or her answer during palpation. It’s difficult to talk and voluntarily guard at the same time. If the pain is real, the patient will stop talking during guarding.
- Avoid gross tests for rebound tenderness, which require pressure and quick release.
They are not precise and are very uncomfortable. Light percussion is just as informative.
- Any pain elicited in the obese patient is significant.
- The physical examination consists of vital signs, inspection, auscultation, light touch, palpation, percussion, and rectovaginal exam
Vital signs
- Note pulse rate and rhythm, blood pressure, temperature, respiratory rate, and the characteristics of the respiratory cycle.
- Painful abdominal conditions frequently are reflected in the vital signs as tachycardia, tachypnea, elevated temperature, and, in conditions that involve the upper abdomen (inflammatory diseases) or the lower lobes of the lung, respiration that is rapid, shallow, painful (grunting), or splinted.
- Hypotension can result from gastrointestinal bleeding, dehydration, vagal stimulation, etc.
Inspection
- Note any abdominal asymmetry, distension, bulges, scars, or splinting of the chest or abdomen during respiration.
- Short, grunting respirations can indicate basilar pneumonia or upper-abdominal inflammatory conditions
Auscultation
- Use either the bell or diaphragm and minimal pressure.
- Auscultate in all four quadrants, and be patient—it may take 2 to 3 minutes in each area to adequately evaluate the nature and character of peristalsis.
- Hyperperistalsis with rushes, cramps, and diarrhea suggests gastroenteritis.
Hypoperistalsis or a silent abdomen favors serious surgical conditions
Light touch
- Gently stroke the abdomen. Underlying peritoneal irritation causes light touch to be perceived as dysesthesia, or a disagreeable sensation, and suggests a surgical process
Palpation
- This procedure should be gentle; applying slow pressure is essential. Palpate for hernias (epigastric, umbilical, incisional, inguinal, femoral, and spigelian) and areas of maximal tenderness. A rigid abdomen indicates a surgical condition.
- If the response to palpation seems exaggerated, repeat auscultation using the diaphragm and more pressure. If the responses have been exaggerated, this maneuver can distract the patient and allow deeper palpation than when done with the hand alone Percussion
- Gentle percussion can detect tympany dullness (ascites) and can isolate the area of maximal discomfort as accurately as the more gross tests of rebound tenderness do
Rectal exam
- Once privacy is ensured, examining the rectum is especially important if the patient has hypogastric pain
- The rectal exam can reveal diffuse tenderness or localized bulges or tenderness associated with abscesses, appendicitis, seminal vesiculitis, or prostatitis. Note the character of the stool; mucoid or jellylike stool often indicates inflammatory bowel disease
Pelvic exam
- Parametrial bulges, masses, and induration favor surgical diagnoses
- Exquisite pain with cervical manipulation, with fever, and without lateralizing signs suggests pelvic inflammatory disease, especially if the patient also has a cervical discharge.
Diagnostic tests
- blood and urine examinations;
- blood chemistry;
- x-rays, including supine and upright views;
- IV urography;
- ultrasound;
- CT;
- arteriography.
- Each has specific indications depending on the disease under consideration.
- However, the most important diagnostic measure in patients with severe abdominal pain often is expeditious exploratory laparotoy
Differential Diagnosis
- Gastroenteritis is likely if family members or associates have had recent similar complaints. Symptoms include colicky pain, nausea, vomiting, and diarrhea, which may be accompanied by mild abdominal tenderness that never becomes localized. Gastroenteritis is self-limited.
- Inflammatory bowel disease can mimic acute appendicitis
- Diverticulitis can produce similar symptoms (usually in the left lower quadrant).
- Herpes zoster can cause severe pain that precedes the typical rash. The pain can be confusing, particularly if the nerves in the right lower quadrant are involved in a patient whose appendix has not been removed.
- Pneumonia can lead to diffuse abdominal pain without localized abdominal tenderness
- Acute MI may be accompanied by poorly localized abdominal pain
- Drug addiction or withdrawal may produce severe colicky pains that suggest intestinal obstruction.
- Anticoagulant use or severe coughing can lead to a hematoma of the abdominal wall or rupture of the deep epigastric artery or vein, events that produce local pain and tenderness
- Sickle cell disease may cause attacks of severe abdominal pain.
- The most common cause of abdominal pain in spinal cord or CNS disease is radiculitis, which usually produces chronic rather than acute pain.
- Psychogenic somatoform disorders often lead to complaints of attacks of severe abdominal pain for which no organic cause can be found
ASCITES
- The accumulation of excess fluid in the peritoneal cavity is called ascites
- Most common cause: cirrhosis
- Ascites usually becomes clinically detectable when at least 500 mL have accumulated
- The fluid is generally serous, having less than 3 gm/dL of protein (largely albumin)
- The fluid may contain a scant number of mesothelial cells and mononuclear leukocytes
- Influx of neutrophils suggests infection, whereas the presence of blood cells points to possible disseminated intra-abdominal cancer
- Although the mechanisms responsible for the development of ascites are not completely understood, several factors contribute to fluid accumulation, including an increase in capillary pressure due to portal hypertension and obstruction of venous flow through the liver, salt and water retention by the kidney, and decreased colloid osmotic pressure due to impaired synthesis of albumin by the liver
- Diminished blood volume (i.e., underfill theory) and excessive blood volume (i.e., overfill theory) have been used to explain the increased salt and water retention by the kidney.
- According to the underfill theory, a contraction in the effective blood volume constitutes an afferent signal that causes the kidney to retain salt and water. The effective blood volume may be reduced because of loss of fluid into the peritoneal cavity or because of vasodilation caused by the presence of circulating vasodilating substances.
- The overfill theory proposes that the initial event in the development of ascites is renal retention of salt and water caused by disturbances in the liver itself
- These disturbances include failure of the liver to metabolize aldosterone, causing an increase in salt and water retention by the kidney
- Another contributing factor in the pathogenesis of ascites is a decreased colloidal osmotic pressure, which limits reabsorption of fluid from the peritoneal cavity
SIGNS OF ASCITES
- Increase in abdominal girth and weight gain
- Everted umbilicus
- Scrotal edema
- Bulging flanks when patient lying supine
- Tympany over the umbilicus and dullness over the lateral abdomen and flank areas upon percussion
- Positive fluid wave test or shifting dullness test
- Signs and symptoms of the esophagus diseases, methods examination of the esophagus.
- The esophagus is a hollow, muscular tube coursing through the posterior mediastinum joining the hypopharynx to the stomach with a sphincter at each end.
- It functions to transport food and fluid between these ends, otherwise remaining empty.
- Esophageal diseases can be manifested by impaired function or pain.
- Key functional impairments are swallowing disorders and excessive gastroesophageal reflux.
- Pain, sometimes indistinguishable from cardiac chest pain, can result from inflammation, infection, dysmotility, or neoplasm.
| Major symptoms | |
| Heartburn (pyrosis) |
(GERD) is so strong that empirical therapy for GERD has become accepted |
| Regurgitati on |
|
| Chest pain | – | common symptom with characteristics similar to cardiac pain |
| – | a pressure type sensation in the mid chest, radiating to the mid back, arms, or jaws. | |
| – | similarity to cardiac pain because the two organs share a nerve plexus and the nerve endings in the esophageal wall have poor discriminative ability among stimuli. | |
| – | Esophageal distention or even chemostimulation (e.g., with acid) will often be perceived as chest pain. | |
| – | Gastroesophageal reflux is the most common cause of esophageal chest pain. | |
| Esophagea l dysphagia | –
– | a feeling of food “sticking” or even lodging in the chest.
Important distinctions are between uniquely solid food dysphagia as opposed to liquid and solid, episodic versus constant dysphagia, and progressive versus static dysphagia. |
| – | If the dysphagia is for liquids as well as solid food, it suggests a motility disorder such as achalasia. Conversely, uniquely solid food dysphagia is suggestive of a stricture, ring, or tumor. | |
| – | Of note, a patient’s localization of food hang-up in the esophagus is notoriously imprecise. Approximately 30% of distal esophageal obstructions are perceived as cervical dysphagia. In such instances, the absence of concomitant symptoms generally associated with oropharyngeal dysphagia such as aspiration, nasopharyngeal regurgitation, cough, drooling, or obvious neuromuscular compromise should suggest an esophageal etiology. | |
| Odynophag
ia | –
– | is pain either caused by or exacerbated by swallowing.
may manifest concurrently with dysphagia. |
| – | more common with pill or infectious esophagitis than with reflux esophagitis and should prompt a search for these entities. When odynophagia does occur in GERD, it is likely related to an esophageal ulcer or extensive erosions. | |
| Globus sensation (globus pharyngeus
/hystericus) |
Clinical experience teaches that it is often attributable to GERD. | |
| Water brash |
|
- Upper endoscopy-Direct visualization of the esophageal lining will allow a check for potential damage (esophagitis, ulcers).
- Biopsy
- Esophagram- swallows barium radiologist visualizes the esophagus and stomach under fluoroscopy.
- Esophageal Manometry- This test involves a small diameter tube passed through the nose into the esophagus. The nose and throat of the patient are numbed prior to this procedure. Once the tube is in position, the patient is asked to swallow. Measurements of esophageal function are made by the use of pressure readings of the muscle contractions
- Signs and symptoms of the stomach diseases, methods of examination of the stomach
The stomach is a saccular organ located in the upper abdomen. The lumen is continuous with the esophagus at the GE junction and with the duodenum at the pyloric sphincter.
The stomach is divided into five anatomic regions. The cardia is the most proximal region of the stomach and extends a very short distance from the GE junction (usually <5 mm). The fundus is the dome-shaped upper portion of the stomach, located to the left and above the GE junction. The body, or corpus, makes up the majority of the stomach and extends from the fundus to the antrum. The antrum makes up the distal third of the stomach and extends to the pylorus/pyloric sphincter, which is surrounded by a smooth muscle layer that controls the passage of food from the stomach to the duodenum. The gastric rugae are a series of mucosal folds that are prevalent in the fundus and body and allow the stomach to expand with a meal.
Gastrointestinal (GI) diseases most often present with one or more of four common classes of symptoms and signs:
- abdominal or chest pain
- altered ingestion of food (eg, resulting from nausea, vomiting, dysphagia [difficulty swallowing], odynophagia [painful swallowing], or anorexia [lack of appetite])
- altered bowel movements (ie, diarrhea or constipation)
- GI tract bleeding, either occurring without warning or preceded by one or more of the foregoing.
However, not all cases of a particular GI disease present in the same way. For example, peptic ulcer disease, although typically accompanied by abdominal pain, may be painless.
There are many tools for investigating stomach problems. The most common is endoscopy. This procedure is performed as an outpatient and utilizes a small flexible camera. The procedure does require intravenous sedation and takes about 30–45 minutes; the endoscope is inserted via the mouth and can visualize the entire swallowing tube, stomach and duodenum. The procedure also allows the physician to obtain biopsy samples. In many cases of bleeding, the surgeon can use the endoscope to treat the source of bleeding with laser, clips or other injectable drugs.Other radiological studies frequently used to assess patients with chronic stomach problems include a barium swallow, where a dye is consumed and pictures of the esophagus and stomach are obtained every few minutes. Other tests include a 24-hour pH
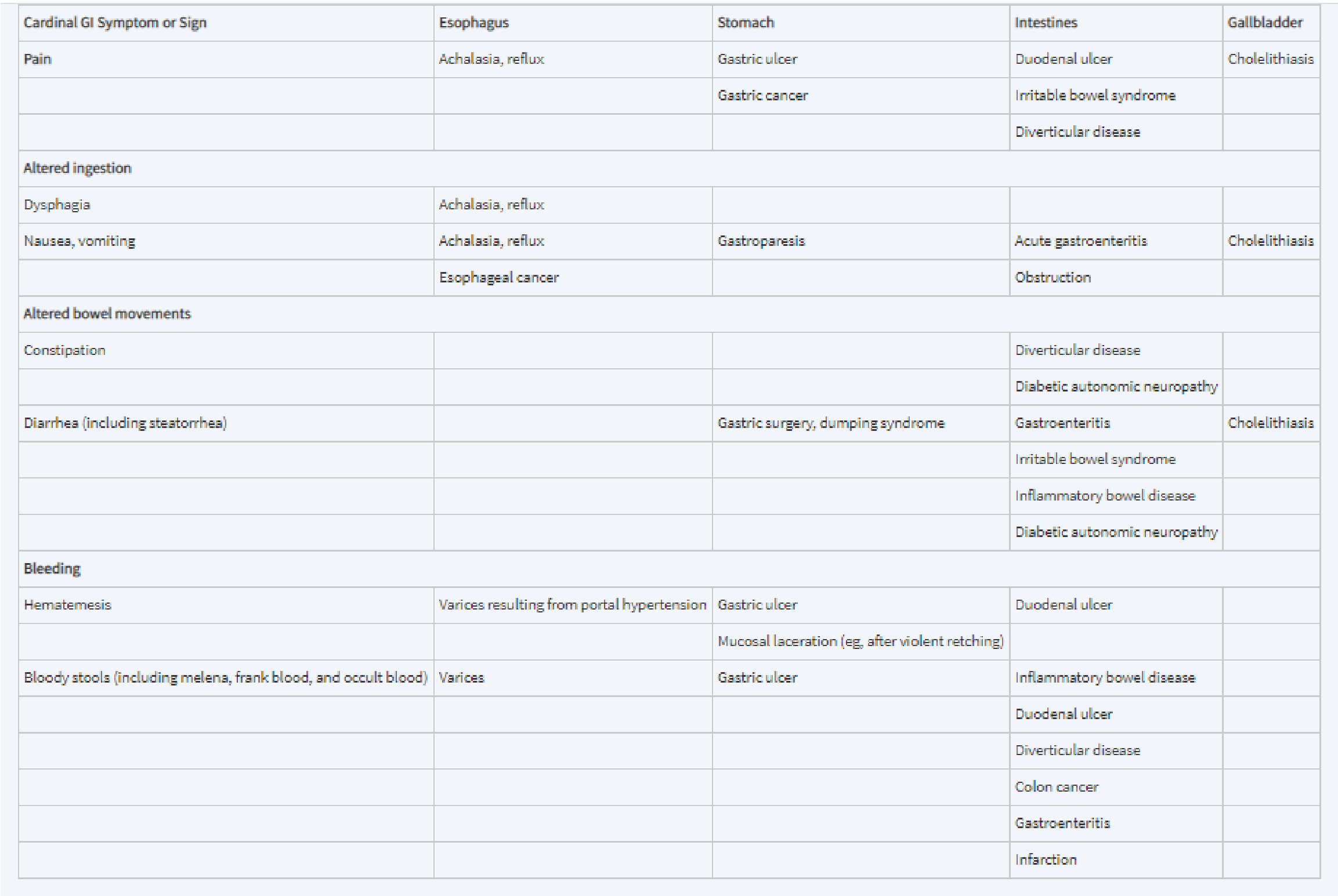
study, CT scans or MRI etc.
ABDOMINAL EXAMINATIONS ARE ALSO USED TO INVESTIGATE.
41. Diarrhea. Constipation. Melena.
Constipation
- is a condition of the digestive system where an individual has hard feces that are difficult to expel.
- may accompany any abdominal condition that causes an illness
- Obstipation —non passage of both stool and gas— however, always suggests a surgical problem Causes:
1. Lack of fiber in the diet + Not drinking enough water 2. Physical inactivity
Especially for old people. For individuals who have been bedridden for a long time, perhaps for several days or weeks,their risk of having constipation is significantly increased.
3. Medications
-The most common medications to cause constipation are:
-Narcotic (opioid) pain drugs including codeine (Tylenol), oxycodone (Percocet), and hydromorphone (Dilaudid)
-Antidepressants including amitriptyline (Elavil) and imipramine (Tofranil)
-Anticonvulsants including phenytoin (Dilantin) and carbamazepine (Tegretol) iron Supplements
-Calcium channel blocking drugs including diltiazem (Cardizem) and nifedipine
(Procardia) -Diuretics including chlorothiazide (Diuril)
4. Inflammatory bowel syndrome 5. Pregnancy
– the uterus may compress the intestine, slowing down the passage of food.
6. Problems with the colon or rectum
- Tumors can compress or restrict the passages and cause constipation
- Scar tissue, diverticulosis, and abnormal narrowing of the colon or rectum, known as colorectal stricture.
- People with Hirschsprung disease are susceptible to constipation (a birth defect in which some nerve cells are absent in the large intestine).
Symptoms:
-Stool is often hard and dry
-Other symptoms may include abdominal pain, bloating, and feeling as if one has not completely passed the bowel movement
Diarrhea
Def: a condition in which feces are discharged from the bowels frequently and in a liquid form Causes:
Acute Diarrhea
-Most common in children are Rotavirus and in adults are Norovirus (viral gastroenteritis) -Bacteria ( E.Coli) is a common cause of traveler’s diarrhea.
Chronic Diarrhea
Fatty or malabsorption:
-impaired digestion of fats due to low pancreatic enzyme levels and impaired absorption of fats due to small bowel disease
-due to chronic pancreatitis which is a result of chronic injury to the pancreas or result of alcohol abuse
-Inflammatory diseases: inflammatory bowel disease (IBD), which is ulcerative colitis or Crohn’s disease.
-Less common causes: ischemia of the gut, radiation therapy and colon cancer or polyps -Infections leading to chronic diarrhea are uncommon, with the exception of parasites
Symptoms:
- abdominal cramps fever, nausea, vomiting, fatigue and urgency
- Chronic diarrhea can be accompanied by weight loss, malnutrition, abdominal pain or other symptoms of the underlying illness.
- Clues for organic disease are weight loss, diarrhea that wakes you up at night, or blood in the stools.
- Diarrhea especially with cramps, indicates gastroenteritis and other nonsurgical conditions like inflammatory bowel disease
Diagnostic
Acute diarrhea:
- resolve quickly in 48h without antibiotic therapy and with simple dietary modifications Chronic diarrhea:
- Blood count look for anemia and infections, an electrolyte and kidney function panel to assess for electrolyte abnormalities and renal insufficiency, and albumin to assess your nutritional status
- Stool sample define the type of diarrhea (fatty, inflammatory, or watery diarrhea) – Culture: a bacterial culture and ova/parasite studies of a stool specimen will also help determine if an infectious etiology is present
- Endoscopic examination of the colon with flexible sigmoidoscopy or colonoscopy and upper endoscopy detecting the etiology of chronic diarrhea
-Biopsies for microscopic evaluation
-Double-balloon enteroscopy and capsule endoscopy
- Ultrasound and CT scan of the abdomen can be helpful to evaluate the bowel, pancreas and other intra-abdominal organs.
Melena
- tar black diarrhea
The black color and characteristic strong odor are caused by hemoglobin in the blood being altered by digestive enzymes and intestinal bacteria. In blood loss from the upper GI tract below the esophagus Causes:
- Most common cause of melena is peptic ulcer disease
- But, any bleeding within the upper gastrointestinal tract or the ascending colon can lead to melana
- Melena may also be a complication of anticoagulant medications, such as warfarin – Malignant tumors affecting the esophagus, stomach or small intestine, hemorrhagic blood diseases, such as thrombocytopenia and hemophilia, gastritis, esophageal varices, Meckel’s diverticulum and Mallory-Weiss syndrome
- Peptic ulcer disease
- Esophageal varices
- Gastric cancer
- A less serious, self-limiting case of melena can occur in newborns two to three days after delivery, due to swallowed maternal blood.
Hematochezia
-blood in stool
- is the passage of fresh blood through the anus, usually in or with stools (contrast with melena)
- Hematochezia is commonly associated with lower gastrointestinal bleeding – The difference between hematochezia and rectorrhagia is that, in the latter, rectal bleeding is not associated with defecation; instead, it is associated with expulsion of fresh bright red blood without stools Causes:
- Colorectal cancer, Crohn’s disease, Ulcerative colitis
- Other types of inflammatory bowel disease, inflammatory bowel syndrome, or ulceration
- Rectal or anal hemorrhoids or anal fissures, particularly if they rupture or are otherwise irritated[citation needed]
- Shigella or shiga toxin production , E. coli food poisoning
- Necrotizing enterocolitis
- Diverticulosis
- Salmonellosis
Hematemesis
- coffee residue appearance of vomiting
- is the vomiting of blood where the source is the upper gastrointestinal tract, typically above the suspensory muscle of duodenum
42. Maldigestion and malabsorption syndromes
Impaired digestion and re-absorption of fats in the gastrointestinal tract
Malassimilation: is a reduced nutrient utilization in the gastrointestinal tract. Two disorders are distinguished:
- Maldigestion: is a disorder of intraluminal splitting (digestion) of supplied nutrients
- Causes: pancreatic diseases (ex: chronic pancreatitis, cystic fibrosis) =pancreatic enzymes (colipase,trypsinogen, bile salts etc) are missing or cannot reach the small intestine through bile duct obstruction
- Malabsorption: is due to disorders of enterocytic membrane transport, resulting in poor absorption of the dietary constituents and their digestive cleavage products
Primary malabsorption syndromes
- They are usually hereditary and are therefore also referred to as congenital disorders of intestinal absorption
- These are singular resorption disorders that are based on an enzyme defect in the area of the brush border of the enterocytes
Secondary malabsorption syndromes
- They are usually acquired and represent a broad spectrum of differential diagnostic diseases
- Diseases with secondary malabsorption are (Ex. Celiac disease, tropical sprue, intestinal lymphangiectasia, immune deficiency syndromes, eosinophilic gastroenteritis,
mastocytosis, amyloidosis, parasitic intestinal colonization, intestinal deficient blood flow (ischemia), radiation damage)
Dietary Insufficiency – Malnutrition
- Malnutrition, also referred to as protein energy malnutrition or PEM, is a consequence of inadequate intake of proteins and calories, or deficiencies in the digestion or absorption of proteins, resulting in the loss of fat and muscle tissue, weight loss, lethargy, and generalized weakness
- Appropriate diet should provide:
- sufficient energy, in the form of carbohydrates, fats, and proteins, for the body’s daily metabolic needs
- amino acids and fatty acids to be used as building blocks for synthesis of proteins and lipids
- vitamins and minerals, which function as coenzymes or hormones in vital metabolic pathways or, as in the case of calcium and phosphate, as important structural components
- In primary malnutrition, one or all of these components are missing from the diet
- By contrast, in secondary malnutrition, malnutrition results from malabsorption, impaired utilization or storage, excess loss, or increased need for nutrients
- Several conditions that may lead to primary or secondary malnutrition:
- Poverty
- Infections
- Acute and chronic illnesses
- The basal metabolic rate becomes accelerated in many illnesses resulting in increased daily requirements for all nutrients. Failure to recognize these nutritional needs may delay recovery
- Chronic alcoholism
- Alcoholic persons may sometimes suffer PEM but more frequently have deficiencies of vitamins, especially thiamine, pyridoxine, folate, and vitamin A, as a result of poor diet, 25 defective gastrointestinal absorption, abnormal nutrient utilization and storage, increased metabolic needs, and an increased rate of loss.
- Ignorance and failure of diet supplementation
- Self-imposed dietary restriction. Anorexia nervosa, bulimia
- Other causes. Additional causes of malnutrition include gastrointestinal diseases and malabsorption syndromes, genetic diseases, specific drug therapies (which block uptake or utilization of particular nutrients), and inadequate total parenteral nutrition.
Protein-Energy Malnutrition
- Severe PEM is a serious, often lethal disease that preferentially affects children.
- Malnutrition is determined according to the body mass index (BMI, weight in kilograms divided by height in meters squared)
- BMI less than 16 kg/m² is considered malnutrition (normal range 18.5 to 25 kg/ m²)
- A child whose weight falls to less than 80% of normal (provided in standard tables) is considered malnourished
- The two ends of the spectrum of PEM syndromes are known as marasmus (calorie deficiency) and kwashiorkor (protein deficiency)
- From a functional standpoint, there are two differentially regulated protein compartments in the body:
- somatic compartment, represented by proteins in skeletal muscles
- visceral compartment, represented by protein stores in the visceral organs, primarily the liver
- —> Somatic compartment is affected more severely in marasmus, and the visceral compartment is depleted more severely in kwashiorkor
Marasmus
- when weight falls to 60% of normal for sex, height, and age
- leads to growth retardation and loss of muscle, the latter resulting from catabolism and depletion of the somatic protein compartment
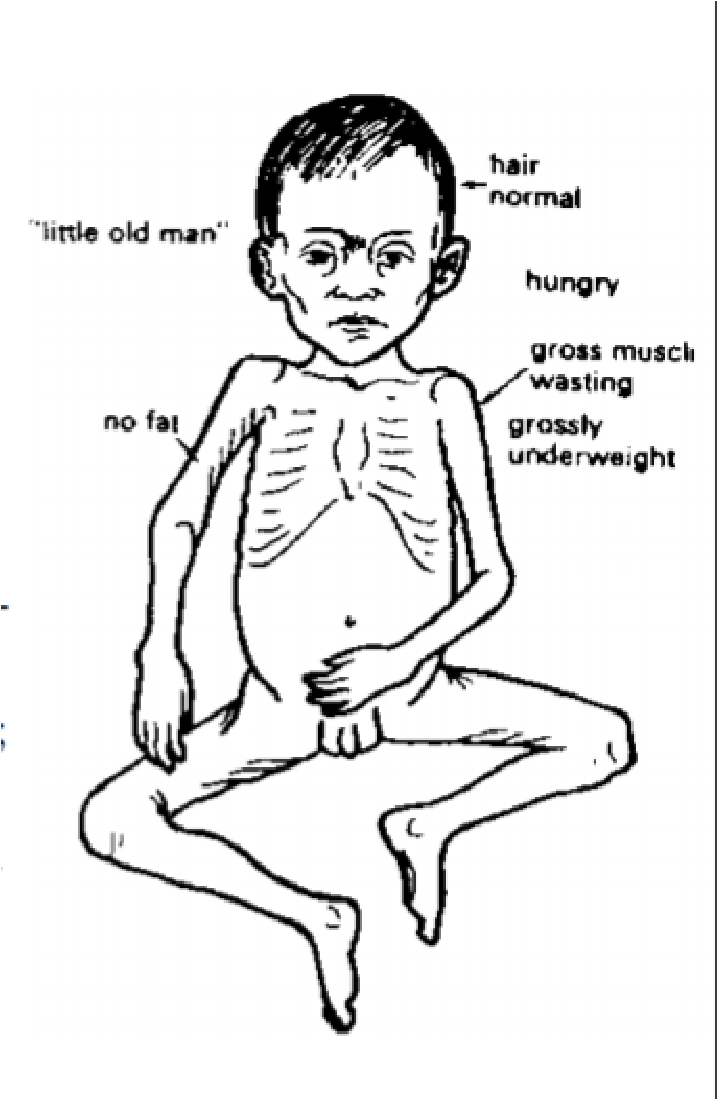 The visceral protein compartment, which is presumably more precious and critical for survival, is only marginally depleted, and hence serum albumin levels are either normal or only slightly reduced.
The visceral protein compartment, which is presumably more precious and critical for survival, is only marginally depleted, and hence serum albumin levels are either normal or only slightly reduced.- In addition to muscle proteins, subcutaneous fat is also mobilized and used as fuel production of leptin is low, which may stimulate the hypothalamic-pituitary adrenal axis to produce high levels of cortisol that contribute to lipolysis
- Due to losses of muscle and subcutaneous fat, the extremities are emaciated; by comparison, the head appears too large for the body
- Anemia and manifestations of multiple vitamin deficiencies are present, and there is evidence of immune deficiency, particularly T-cell–mediated immunity
- Hence, concurrent infections are usually present, which impose additional nutritional demands
Kwashiorkor
- protein deprivation is relatively more severe than the deficit in total calories
- Associated with severe depletion of the visceral protein compartment, and the resultant hypoalbuminemia gives rise to generalized or dependent edema
- Loss of weight in these patients is masked by the increased fluid retention
- In further contrast to marasmus, there is relative sparing of subcutaneous fat and muscle mass
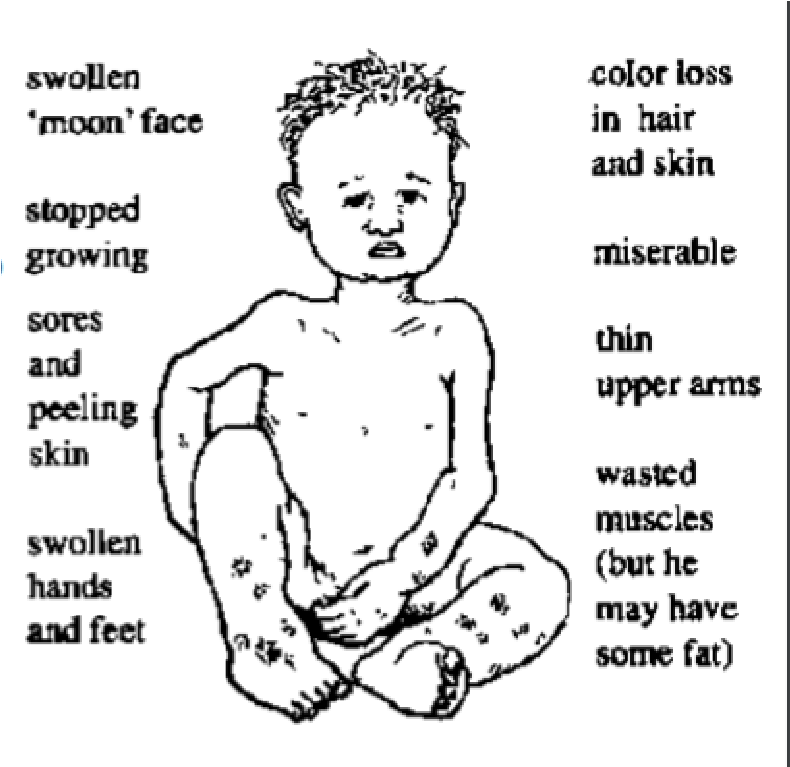 Children with kwashiorkor have characteristic skin lesions, with alternating zones of hyperpigmentation, areas of desquamation, and hypopigmentation, giving a “flaky paint” appearance
Children with kwashiorkor have characteristic skin lesions, with alternating zones of hyperpigmentation, areas of desquamation, and hypopigmentation, giving a “flaky paint” appearance- Hair changes include overall loss of color or alternating bands of pale and darker hair.
- Other features that differentiate kwashiorkor from marasmus include an enlarged, fatty liver (resulting from reduced synthesis of the carrier protein component of lipoproteins), and the development of apathy, listlessness, and loss of appetite
Vitamin deficiencies are likely to be present, as are
defects in immunity and secondary infections
- Compromised fluid recovery results in the characteristic belly distension observed in highly malnourished children
Morphology
- main anatomic changes in PEM are
- growth failure
- peripheral edema in kwashiorkor
- loss of body fat and atrophy of muscle, more marked in marasmus
- liver in kwashiorkor, but not in marasmus, is enlarged and fatty; superimposed cirrhosis is rare
- In kwashiorkor (rarely in marasmus) the small bowel shows a decrease in the mitotic index in the crypts of the glands, associated with mucosal atrophy and loss of villi and microvilli. In such cases concurrent loss of small intestinal enzymes occurs, most often manifested as disaccharidase deficiency
- Bone marrow in both kwashiorkor and marasmus may be hypoplastic, mainly as a result of decreased numbers of red cell precursors
- Peripheral blood commonly reveals mild to moderate anemia, which is often multifactorial in origin; nutritional deficiencies of iron, folate, and protein, as well as the suppressive effects of infection (anemia of chronic disease) may all contribute.
- Depending on the predominant factor, the red cells may be microcytic, normocytic, or macrocytic
- Brain in infants who are born to malnourished mothers and who suffer PEM during the first 1 or 2 years of life has been reported by some to show cerebral atrophy, a reduced number of neurons, and impaired myelinization of white matter
- Other: thymic and lymphoid atrophy (more marked in kwashiorkor than in marasmus); anatomic alterations induced by intercurrent infections, particularly with all manner of endemic worms and other parasites; deficiencies of other required nutrients such as iodine and vitamins
Cachexia
- Highly debilitating condition characterized by extreme weight loss, fatigue, muscle atrophy, anemia, anorexia, and edema
- Mortality is generally the consequence of atrophy of the diaphragm and other respiratory muscles
- Common complication in patients with AIDS or advanced cancers
- Causes of cachexia are not known, but it is clear that mediators secreted by tumors and during chronic inflammatory reactions contribute to its development
Anorexia Nervosa and Bulimia
- Anorexia nervosa is self-induced starvation, resulting in marked weight loss
Bulimia is a condition in which the patient binges on food and then induces vomiting.
- Anorexia nervosa has the highest death rate of any psychiatric disorder
- Bulimia is more common than anorexia nervosa, and generally has a better prognosis
- Both occur primarily in previously healthy young women who have developed an obsession with body image and thinness; neurobiological underpinnings are unknown, altered serotonin metabolism may be an important component
- In anorexia nervosa, clinical findings are generally similar to those in severe PEM. In addition, effects on the endocrine system are prominent
- Amenorrhea (absence of menstruation), resulting from decreased secretion of gonadotropin-releasing hormone, and subsequent decreased secretion of luteinizing hormone and follicle-stimulating hormone, is so common that its presence is considered a diagnostic feature
- Findings related to decreased thyroid hormone release include cold intolerance, bradycardia, constipation, and changes in the skin and hair
- Dehydration and electrolyte abnormalities are frequently present. The skin becomes dry and scaly
- Bone density is decreased, most likely because of low estrogen levels, mimicking the post- menopausal acceleration of osteoporosis
- Anemia, lymphopenia, and hypoalbuminemia may be present
- Increased susceptibility to cardiac arrhythmia and sudden death, resulting from hypokalemia
- In bulimia, binge eating is the normal
- Large amounts of food, principally carbohydrates, are ingested, only to be followed by induced vomiting
- Although menstrual irregularities are common, amenorrhea occurs in less than 50% of bulimic patients because weight and gonadotropin levels remain near normal
- major medical complications related to frequent vomiting and the chronic use of laxatives and diuretics:
▪ electrolyte imbalances (hypokalemia), which predispose the patient to cardiac arrhythmias
▪ pulmonary aspiration of gastric contents
▪ esophageal and gastric rupture
▪ tooth enamel erosion
Diagnosis of bulimia relies on a comprehensive psychological assessment of the person
- Signs and symptoms of the colon diseases. Methods of examination of the colon.
Signs and Symptoms (Colitis)
- Tenesmus,
- Blood and mucus in stool
Fever, Chills, Fatigue,
- Changes in bowel habits (increased frequency),
- Tenderness in the abdomen,
- Rapid weight loss,
- Swelling of the colon tissue,
- Ulcers on the colon, ● Constipation,
- Pains within the joints.
Complications
Penetration, Fistula formation, Abscess formation, Dehydration, Perforation, Blood loss
Physical examination
The physical examination consists of vital signs, inspection, auscultation, light touch, palpation, percussion, and rectovaginal exam ➔ Vital signs.
-
- Note pulse rate and rhythm, blood pressure, temperature, respiratory rate, and the characteristics of the respiratory cycle.
- Painful abdominal conditions frequently are reflected in the vital signs as tachycardia, tachypnea, elevated temperature, and, in conditions that involve the upper abdomen (inflammatory diseases) or the lower lobes of the lung, respiration that is rapid, shallow, painful (grunting), or splinted.
- Hypotension can result from gastrointestinal bleeding, dehydration, vagal stimulation, etc.
– Gentle percussion can detect tympany dullness (ascites) and can isolate the area of maximal discomfort as accurately as the more gross tests of rebound tenderness do
- Rectal exam
- Once privacy is ensured, examining the rectum is especially important if the patient has hypogastric pain.
- The rectal exam can reveal diffuse tenderness or localized bulges or tenderness associated with abscesses, appendicitis, seminal vesiculitis, or prostatitis.
- Note the character of the stool; mucoid or jellylike stool often indicates inflammatory bowel disease. ➔ Pelvic exam
- Parametrial bulges, masses, and induration favor surgical diagnoses.
- Exquisite pain with cervical manipulation, with fever, and without lateralizing signs suggests pelvic inflammatory disease, especially if the patient also has a cervical discharge.
Diagnostic tests
○ blood and urine examinations;
○ blood chemistry;
○ x-rays, including supine and upright views;
○ IV urography;
○ Ultrasound;
○ CT;
○ Arteriography
○ Each has specific indications depending on the disease under consideration.
○ However, the most important diagnostic measure in patients with severe abdominal pain often is expeditious exploratory laparotomy.
For colon cancer:
- Digital rectal exam
- Fecal occult blood test (FOBT)
- Endoscopy & biopsy
- Double contrast barium enema (DCBE)
- Virtual colonoscopy
- carcinoembryonic antigen (CEA)
- Positron emission tomography (PET)
- Liver failure
There are two types of live failure:
- Acute: This is when your liver stops working within a matter of days or weeks. Most people who get this don’t have any type of liver disease or problem before this event.
- Chronic: Damage to your liver builds up over time and causes it to stop working.
Acute liver failure
Acute liver failure – development of hepatic encephalopathy (confusion, stupor and coma) and decreased production of proteins (such as albumin and blood clotting proteins) within four weeks of the first symptoms (such as jaundice) of a liver problem. “Hyperacute” liver failure is said to be present if this interval is 7 days or less, while “subacute” liver failure is said to be present if the interval is 5-12 weeks.
Overall, the most common causes of acute liver failure are:
● Viruses, primarily hepatitis B ● Drugs and toxins, most commonly acetaminophen
- Vascular disorders
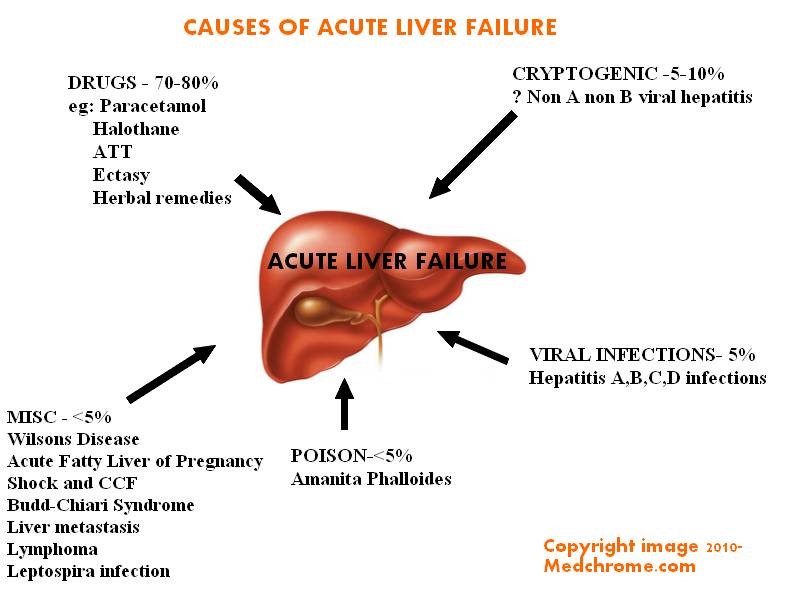 Metabolic disorders Vascular causes include hepatic vein thrombosis (Budd-Chiari syndrome), ischemic hepatitis, portal vein thrombosis, and hepatic sinusoidal obstruction syndrome (also called hepatic venoocclusive disease), which is sometimes drug- or toxin-induced. Metabolic causes include acute fatty liver of pregnancy, HELLP syndrome (hemolysis, elevated values on liver tests, and low platelets),
Metabolic disorders Vascular causes include hepatic vein thrombosis (Budd-Chiari syndrome), ischemic hepatitis, portal vein thrombosis, and hepatic sinusoidal obstruction syndrome (also called hepatic venoocclusive disease), which is sometimes drug- or toxin-induced. Metabolic causes include acute fatty liver of pregnancy, HELLP syndrome (hemolysis, elevated values on liver tests, and low platelets),
Reye syndrome, and Wilson disease. Other causes include autoimmune hepatitis, metastatic liver infiltration, heatstroke, and sepsis. The cause cannot be determined in up to 20% of cases.
Characteristic manifestations are altered mental status (usually part of portosystemic encephalopathy) and jaundice. Other symptoms may be nonspecific (eg, malaise, anorexia) or result from the causative disorder. Fetor hepaticus (a musty or sweet breath odor) and motor dysfunction are common. Tachycardia, tachypnea, and hypotension may occur with or without sepsis. Signs of cerebral edema can include obtundation, coma, bradycardia, and hypertension. Patients with infection sometimes have localizing symptoms (eg, cough, dysuria), but these symptoms may be absent.
Chronic liver failure
Chronic liver failure usually occurs in the context of cirrhosis, itself potentially the result of many possible causes, such as excessive alcohol intake, hepatitis B or C, autoimmune, hereditary and metabolic causes (such as iron or copper overload, Steatohepatitis or non-alcoholic fatty liver disease).
Chronic liver disease in the clinical context is a disease process of the liver that involves a process of progressive destruction and regeneration of the liver parenchyma leading to fibrosis and cirrhosis. “Chronic liver disease” refers to disease of the liver which lasts over a period of six months. It consists of a wide range of liver pathologies which include inflammation (chronic hepatitis), liver cirrhosis, and hepatocellular carcinoma. The entire spectrum need not be experienced.
The list of conditions associated with chronic liver disease is extensive and can be categorised in the following way:
● Viral causes
Hepatitis B
Hepatitis C
Cytomegalovirus (CMV), Epstein Barr virus (EBV), and yellow fever viruses cause acute hepatitis. ● Toxic and drugs
Alcoholic liver disease
Rarely drug induced liver disease from methotrexate, amiodarone, nitrofurantoin and others
Paracetamol (acetaminophen) causes acute liver damage.
● Metabolic
Non-alcoholic fatty liver disease
Haemochromatosis
Wilson’s disease
● Autoimmune response causes
Primary biliary cholangitis (previously known as primary biliary cirrhosis)
Primary sclerosing cholangitis
Autoimmune Hepatitis
● Other
Right heart failure
Chronic liver disease takes several years to develop and the condition may not be recognised unless there is clinical awareness of subtle signs and investigation of abnormal liver function tests.
Testing for chronic liver disease involves blood tests, imaging including ultrasound and a biopsy of the liver. The liver biopsy is a simple procedure done with a fine thin needle under local anaesthesia. The tissue sample is sent to a laboratory where it is examined underneath a microscope.
45. Jaundice – types of jaundice, mechanisms. l$#,+*D(N’^D-(0#”m n’l$#,+*D(’0(C(0″’-1’-/(’&(%%1.’D1%10’1C’”8*,6’,$*%’>(+”6’$,+’”D%(0$(’E./*-(“’1C’-/(’(&(“G’ D$#”(+’>&’+(?1″*-*1,’1C’>*%*0#>*,6’”(D1,+$0&’-1’*,D0($”(+’>*%*0#>*,’%()(%”’*,’-/(’>%11+’ E/&?(09>*%*0#>*,(=*$Gm n’Y%-/1#M/’@1-’g*”($”(6\$#,+*D(’*”’#”#$%%&’$’”&=?-1=’1C’$’#,+(0%&*,M’+*”10+(0m n’@1-(oX%11+’X*%*0#>*,’O()(%”’Y0(’@10=$%%&’Y>1#-’K=MN+O:’l$#,+*D(’*”’”((,’$-’L‘p=MN
+%:’
Mechanism
As RBC are phagocytized by macrophages in the reticuloendothelial system.
Hemoglobin is broken into heme and globin. Globin is broken into AA. Heme is split into Fe and protoporphyrin. Protoporphyrin is split into unconjugated bilirubin, which binds to albumin and is transported to the liver and is converted by uridine glucuronyl transferase into conjugated bilirubin, where it is secreted into the bile duct and is stored in the gallbladder as bile. Bile is converted into urobilinogen by microbes then urobilin and excreted as faces. Some often urobilin is reabsorbed into the blood and goes to the kidneys and liver. The urobilin in the kidney is excreted as urine.
When liver cells are damaged, UCB cannot be converted to CB and serum bilirubin increases as it cannot be excreted.
Causes
Predominantly unconjugated hyperbilirubinemia
- Excess production of bilirubin; hemolytic anemia, resorption of blood from internal hemorrhage, ineffective erythropoiesis eg. in thalassemia.
- Reduced hepatic uptake; drug interference, Gilbert syndrome
- Impaired bilirubin conjugation; physiologic jaundice of newborn
- Breast milk jaundice
- Genetic deficiency of UGT1A1 activity
- Gilbert syndrome
- Diffuse hepatocellular disease
Predominantly conjugated hyperbilirubinemia
- Deficiency of canalicular membrane transporters
- Imparied bile flow from duct obstruction or autoimmune cholangiopathies
Types of jaundice
- Hemolytic jaundice
- The liver has the capacity to conjugate and excrete over 3000mg of bilirubin per day, whereas the normal production of bilirubin is only 300mg/day
-This excess capacity allows the liver to respond to increased heme degradation with a corresponding increase in conjugation and secretion of bilirubin diglucuronide
-However, extensive hemolysis (for example, in patients with Sickle cell anemia, or pyruvate kinase or glucose-6-phosphate dehydrogenase deficiency) may produce bilirubin faster than it can be conjugated. UCB levels in blood become elevated, causing jaundice.
With hemolysis, more CB is made and excreted into the bile, the amount of urobilinogen entering the enterohepatic circulation is increased, and urinary urobilinogen is increased.
- Hepatocellular jaundice:
- Damage to liver cells (for example, in patients with cirrhosis or hepatitis) can cause UCB levels in the blood to increase as a result of decreased conjugation -Urobilinogen is increased in the urine because hepatic damage decreases the enterohepatic circulation of this compound, allowing more to enter the blood, from which it is filtered into the urine
-The urine consequently darkens, whereas stools may be a pale, clay color -Plasma levels of alanine and aspartate transaminases (AST and ALT) are elevated
Neonatal Jaundice
- The majority of newborn infants (60% of full term and 80% of preterm) show a rise in UCB in the first postnatal week (and a transient, “physiologic” jaundice) because the activity of hepatic bilirubin UGT is low at birth (it reaches adult levels in about 4 weeks)
- Because the hepatic machinery for conjugating and excreting bilirubin does not fully mature until about 2 weeks of age, almost every newborn develops transient and mild unconjugated hyperbilirubinemia, termed neonatal jaundice or physiologic jaundice of the newborn
- This may be exacerbated (verschlimmern) by breastfeeding, as a result of the presence of bilirubin-deconjugating enzymes in breast milk – Nevertheless, sustained jaundice in the newborn is abnormal
- Elevated UCB (unconjugated bilirubin), in excess of the binding capacity of albumin (20–25mg/dl), can diffuse into the basal ganglia, cause toxic encephalopathy (kernicterus) and a pathologic jaundice
- Therefore, newborns with significantly elevated bilirubin levels are treated with blue fluorescent light (phototherapy), which converts bilirubin to more polar and, therefore, water-soluble isomers
- These photos isomers can be excreted into the bile without conjugation to glucuronic acid
Note: Because of solubility differences, only UCB crosses the blood brain barrier , and only CB appears in urine
- Viral hepatitis
An increase in both conjugated and unconjugated bilirubin in the blood. As hepatocytes are infected and die they cannot convert unconjugated bilirubin as they line the bile ducts they leak conjugated bilirubin into blood= darker urine.
- Obstructive jaundice (Cholestasis):
-Bile flow is impaired eg. stones, carcinoma, parasites
-In this instance, jaundice is not caused by overproduction of bilirubin or decreased conjugation but, instead, results from obstruction of the common bile duct (extrahepatic cholestasis)
-For example, the presence of a tumor or bile stones may block the duct, preventing passage of CB into the intestine
-Patients with obstructive jaundice experience GI pain and nausea and produce stools that are a pale, clay color
-The liver “regurgitates” CB into the blood (hyperbilirubinemia)
-The CB is eventually excreted in the urine (which darkens upon standing), and is
referred to as “urinary bilirubin.” Urinary urobilinogen is absent -Can lead to pruritus, xanthomas, cholesterolemia, steatorrhea.
46. Portal hypertension – pathogenesis
General data
- Portal hypertension is characterized by increased resistance to flow in the portal venous system and sustained portal vein pressure
- Normally, venous blood returning to the heart from the abdominal organs collects in the portal vein and travels through the liver before entering the vena cava
- The blood pressure in the portal vein system is usually 7-10 mmHg; Increase of this value is called portal hypertension
- Portal hypertension can be caused by a variety of conditions that increase resistance to hepatic blood flow, including prehepatic, intrahepatic obstructions and posthepatic ->
with hepatic referring to the liver lobules rather than the entire liver
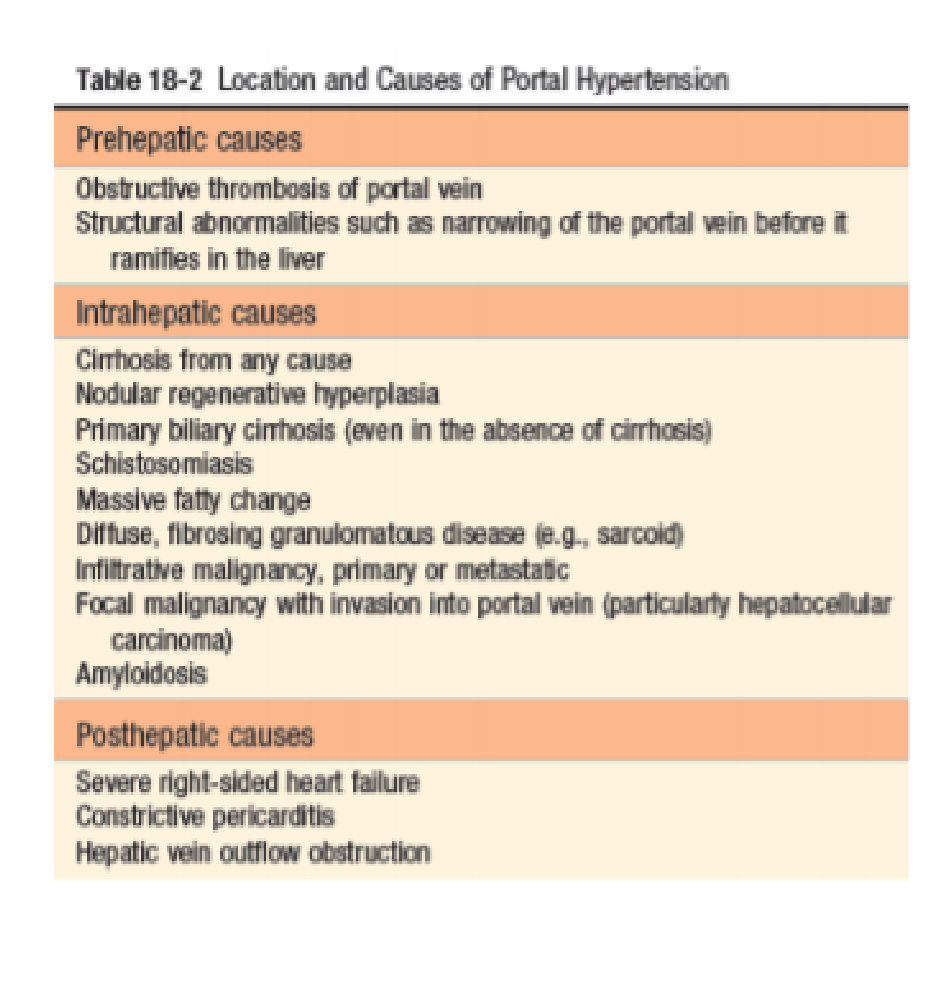 PREHEPATIC PORTAL HYPERTENSION
PREHEPATIC PORTAL HYPERTENSION
- The common causes of pre-hepatic etiology are either due to increased blood flow or obstruction within the portal vein or splenic vein
- Instances of increased blood flow include idiopathic tropical splenomegaly, arterio-venous malformations, or fistula
- A blockage within the portal or splenic vein may be due to thrombosis or to invasion or compression of these veins by the tumor
INTRAHEPATIC PORTAL HYPERTENSION
- In alcoholic cirrhosis, which is the major cause of portal hypertension, bands of fibrous tissue and fibrous nodules distort the architecture of the liver and increase the resistance to portal blood flow, which leads to portal hypertension
- Complications of portal hypertension arise from the increased pressure and dilation of the venous channels behind the obstruction
POSTHEPATIC PORTAL HYPERTENSION
- refers to any obstruction to blood flow through the hepatic veins beyond the liver lobules, either within or distal to the liver
- It is caused by conditions such as thrombosis of the hepatic veins, veno-occlusive disease, and severe right-sided heart failure that impede the outflow of venous blood from the liver
- Budd-Chiari syndrome:
- refers to congestive disease of the liver caused by occlusion of multiple hepatic veins or the hepatic portion of the inferior vena cava
- The principal cause of the Budd-Chiari syndrome is thrombosis of the hepatic veins, in association with diverse conditions such as polycythemia vera, hypercoagulability states associated with malignant tumors, pregnancy, bacterial infection, metastatic disease of the liver, and trauma
- Sinusoidal obstruction syndrome or hepatic veno- occlusive disease is a variant of the BuddChiari syndrome seen most commonly in people treated with certain cancer chemotherapeutic drugs, hepatic irradiation, or bone marrow transplantation
Major clinical consequences of portal hypertension: ascites, formation of portosystemic venous shunts, congestive splenomegaly, and hepatic encephalopathy
![]() Sinusoidal hypertension
Sinusoidal hypertension
- altering Starling’s forces and driving fluid into the space of Disse, from where it is removed by hepatic lymphatics; this movement of fluid is also promoted by hypoalbuminemia
Percolation of hepatic lymph into the peritoneal cavity:
- Normal thoracic duct lymph flow approximates 800 to 1000 mL/day. With cirrhosis, hepatic lymphatic flow may approach 20 L/day, exceeding thoracic duct capacity
- Hepatic lymph is rich in proteins and low in triglycerides, which explains the presence of protein in the ascitic fluid
Splanchnic vasodilation and hyperdynamic circulation
- Arterial vasodilation in the splanchnic circulation tends to reduce arterial blood pressure
- With worsening of the vasodilation, the heart rate and cardiac output are unable to maintain the blood pressure
- This triggers the activation of vasoconstrictors, including the renin-angiotensin system, and increases the secretion of antidiuretic hormone
- The combination of portal hypertension, vasodilation, and sodium and water retention increases the perfusion pressure of interstitial capillaries, causing extravasation of fluid into the abdominal cavity
Portosystemic Shunts:
- With the gradual obstruction of venous blood flow in the liver, the pressure in the portal vein increases, and large collateral channels develop between the portal and systemic veins that supply the lower rectum and esophagus and the umbilical veins of the falciform ligament that attaches to the anterior wall of the abdomen
- The collaterals between the inferior and internal iliac veins may give rise to hemorrhoids
- In some persons, the fetal umbilical vein is not totally obliterated; it forms a channel on the anterior abdominal wall. Dilated veins around the umbilicus are called caput medusae
Portopulmonary shunts:
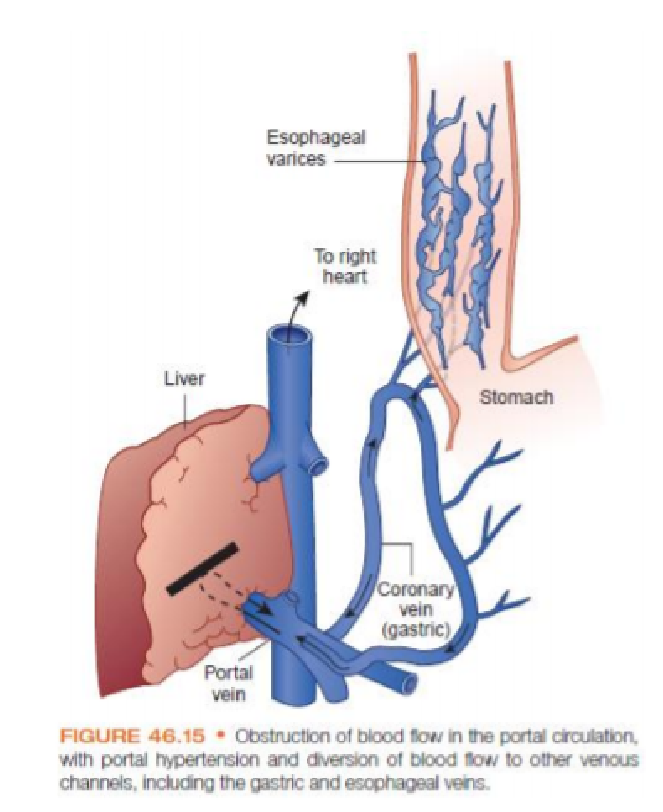 may develop and cause blood to bypass the pulmonary capillaries, interfering with blood oxygenation and producing cyanosis
may develop and cause blood to bypass the pulmonary capillaries, interfering with blood oxygenation and producing cyanosis- Clinically, the most important collateral channels are those connecting the portal and coronary veins that lead to reversal of flow and formation of thin-walled varicosities in the submucosa of the esophagus
- These thin walled esophageal varices are subject to rupture, producing massive and sometimes fatal hemorrhage
- Impaired hepatic synthesis of coagulation factors and decreased platelet levels (i.e., thrombocytopenia) due to splenomegaly may further complicate the control of esophageal bleeding
- Esophageal varices develop in 5% to 15% of people with cirrhosis, and approximately 33% will have bleeding varices
Congestive Splenomegaly:
- The spleen enlarges progressively in portal hypertension because of shunting of blood into the splenic vein
- The enlarged spleen often gives rise to sequestering of significant numbers of blood elements and development of a syndrome known as hypersplenism
- Hypersplenism is characterized by a decrease in the lifespan of all the formed elements of the blood and a subsequent decrease in their numbers, leading to anemia, thrombocytopenia, and leukopenia
- The decreased lifespan of the blood elements is thought to result from an increased rate of removal because of the prolonged transit time through the enlarged spleen.
47. Physical, functional and imaging examination of the liver.
Inspection:
- Skin color-yellow
- Venous collaterals at the lateral aspect of the abdomen or rarely at umbilical area-”caput Medusae”
- Distended and flat abdomen and umbilical hernia in presence of ascites
Percussion:
The purpose of liver percussion is to measure the liver size. ➔ Technique:
- Starting in the midclavicular line at about the 3rd intercostal space, lightly percuss and move down.
- Percuss inferiorly until dullness denotes the liver’s upper border (usually at 5th intercostal space in MCL).
- Resume percussion from below the umbilicus on the midclavicular line in an area of tympany.
- Percuss superiorly until dullness indicates the liver’s inferior border.
- Measure span in centimeters.
➔ Findings:
- Liver span: commonly clinically under estimated.
○ Midclavicular line: normally 6-12cm.
○ Midsternal line: normally 4-8cm.
- False positives for enlarged liver span: right pleural effusion, consolidated lung.
- COPD may depress diaphragm and hence depress liver borders, but not span.
Palpation:
The purpose of liver palpation is to approximate liver size, feel for tenderness and masses. Keep in mind that many of the findings of liver disease are found outside the abdomen.
Technique:
- With patient supine, place right hand on patient’s abdomen, just lateral to the rectus abdominis, well below lower border of liver dullness.
- Ask patient to take a deep breath and try to feel the liver edge as it descends.
- Be sure to allow liver to pass under the fingers of your right hand, note texture. ○ Pressing too hard may interfere.
Findings:
- Tenderness:
○ The normal liver may be slightly tender.
○ Greater tenderness suggests inflammation (e.g. hepatitis) or congestion (e.g.
congestive heart disease).
- Consistency
○ Firm, bluntness/rounding or irregularity of liver edge suggest an abnormality.
○ Obstructed, distended gallbladder may be palpable on the inferior liver edge.
○ Nodules may be palpable; rock hard and umbilicated (central dimple) nodules suggest malignancy.
Functional tests: determine the health of your liver by measuring the levels of proteins, liver enzymes, and bilirubin in your blood.
- Alanine transaminase (ALT) test
- ALT is used to metabolize protein. If the liver is damaged or not functioning properly, ALT can be released into the blood = ALT levels to increase.
- an ALT above 25 IU/L in females and 33 IU/L in males typically requires further testing and evaluation.
- Aspartate aminotransferase (AST) test
- is an enzyme found in several parts of your body, including the heart, liver, and muscles. Since AST levels aren’t as specific for liver damage as ALT, it’s usually measured together with ALT to check for liver problems.
- When the liver is damaged, AST can be released into the bloodstream. A high result on an AST test might indicate a problem with the liver or muscles.
- The normal range for AST is typically up to 40 IU/L in adults and may be higher in infants and young children.
- Alkaline phosphatase (ALP) test
- is an enzyme found in your bones, bile ducts, and liver. An ALP test is typically ordered in combination with several other tests.
- High levels of ALP may indicate liver inflammation, blockage of the bile ducts, or a bone disease.
- Children and adolescents may have elevated levels of ALP because their bones are growing. Pregnancy can also raise ALP levels.
- The normal range for ALP is typically up to 120 U/L in adults.
- Albumin test
- main protein made by your liver. It performs many important bodily functions. For example, albumin:
- stops fluid from leaking out of your blood vessels
- nourishes your tissues
- transports hormones, vitamins, and other substances throughout your body
- An albumin test measures how well your liver is making this particular protein. A low result on this test can indicate that your liver isn’t functioning properly.
- The normal range for albumin is 3.5–5.0 grams per deciliter (g/dL). However, low albumin can also be a result of poor nutrition, kidney disease, infection, and inflammation.
- Bilirubin test
- is a waste product from the breakdown of red blood cells. It’s ordinarily processed by the liver. It passes through the liver before being excreted through your stool.
- A damaged liver can’t properly process bilirubin. This leads to an abnormally high level of bilirubin in the blood. A high result on the bilirubin test may indicate that the liver isn’t functioning properly.
- The normal range for total bilirubin is typically 0.1–1.2 milligrams per deciliter (mg/dL). There are certain inherited diseases that raise bilirubin levels, but the liver function is normal.
Imaging tests of the liver:
- Ultrasound
- Required before liver biopsy
- routine procedure
- provide information about the surface and shape of your liver, and its general appearance, and highlight unexpected changes or anything that is not normal.
- Info:
- Evaluating the hepatobiliary tract in patients with right upper quadrant abdominal pain
- Differentiating intrahepatic from extrahepatic causes of jaundice
- Screening for liver masses
- Elastography( FibroScan)
- similar to ultrasound, measures the stiffness of the liver.
- Healthy liver tissue is soft, stiffness = fibrosis (scar tissue) may be present.
- can’t diagnose specific liver diseases but they can give doctors an idea of how badly the liver is damaged.
- Sheer wave elastography (SWE)
- advanced version elastography, uses a focused ultrasound wave to give radiologists a clearer picture of how ‘elastic’ (soft) the liver is.
- The waves travel slowly through healthy liver tissue and faster through scarred areas.
- Acoustic radiation force impulse imaging (ARFI) = works by ‘pushing’ tissues to assess their stiffness – softer, healthy tissue is more easily pushed than stiffer tissue, which may indicate fibrosis.
- CT scan (computed tomography scan)
- useful for showing several types of tissue very clearly – lungs, bones, soft tissues and blood vessels.
- particularly useful in detecting excess fat in the liver (fatty liver).
- MRI (magnetic resonance imaging)
- provides a more detailed view of organs than a CT.
- very useful for investigating tumours both before and after treatment.
- A type of MRI scan called Liver MultiScan is sometimes used to accurately measure the amount of fat, fibrosis (scarring) and inflammation present in the liver.
- MRCP (magnetic resonance cholangiopancreatography)
- Uses specialised magnetic resonance imaging (MRI) to provide a picture biliary and pancreatic ducts. The fluid biliary ducts appear brighter while the surrounding organs and tissues will appear darker.
- Used to find any lodged gallstones in any of the ducts surrounding your gallbladder.
- X-rays
- A special X-ray that studies the veins and arteries that supply blood to the liver is known as hepatic angiography.
- Needed if diagnosis is still doubtful after a CT and MRI scan.
48.Signs and symptoms of pancreatitis. Physical and functional examination of the pancreas.
Signs
- The main presentation of acute pancreatitis is epigastric pain or right upper quadrant pain radiating to the back
- Nausea and/or vomiting
- Fever
- Query the patient about recent surgeries and invasive procedures (ie, endoscopic retrograde cholangiopancreatography) or family history of hypertriglyceridemia
- Patients frequently have a history of previous biliary colic and binge alcohol consumption, the major causes of acute pancreatitis.
Physical Examination
- Tachycardia, Tachypnea, Hypotension, Fever,
- Abdominal tenderness, distension, guarding, and rigidity
- Mild jaundice, Diminished or absent bowel sounds
- Because of contiguous spread of inflammation (effusion) from the pancreas, lung auscultation may reveal basilar rales, especially in the left lung.
- Occasionally, in the extremities, muscular spasm may be noted secondary to hypocalcemia.
- Severe cases may have a Grey Turner sign (ie, bluish discoloration of the flanks) and Cullen sign (ie, bluish discoloration of the periumbilical area) caused by the retroperitoneal leak of blood from the pancreas in hemorrhagic pancreatitis.
Differential Diagnosis (DD)
- Abdominal aneurysm
- Cholangitis , Cholecystitis and Biliary Colic , Cholelithiasis, Choledocholithiasis
- Gastroenteritis
- Hepatitis
- Mesenteric Ischemia
- Large Bowel Obstruction, Small Bowel Obstruction
- Perforated viscus, Acute peritonitis
- Macroamylasemia, Macrolipasemia
- Intestinal obstruction
- Pancreatic cancer, Malabsorption syndromes/processes
Laboratory Tests
- A complete blood count (CBC) demonstrates leukocytosis (WBC >12000)
- If blood transfusion is necessary, as in cases of hemorrhagic pancreatitis, obtain type and crossmatch.
- Measure blood glucose level because it may be elevated from B cell injury in the pancreas.
- Obtain measurements for BUN, creatine (Cr), and electrolytes (Na, K, Cl, CO2, P, Mg); a great disturbance in the electrolyte balance is usually found, secondary to third spacing of fluids.
- Measure amylase levels, preferably the Amylase P, which is more specific to pancreatic pathology. Levels more than 3 times higher than normal strongly suggest the diagnosis of acute pancreatitis
- Lipase levels also are elevated and remain high for 12 days. In patients with chronic pancreatitis (usually caused by alcohol abuse), lipase may be elevated in the presence of a normal serum amylase level
- Perform liver function tests and bilirubin, particularly with biliary origin pancreatitis.
Imaging studies
Perform a plain KUB (Kidneys, ureters, bladder) with the patient in the upright position to exclude viscus perforation (ie, air under the diaphragm). In cases with a recurrent episode of chronic pancreatitis, peripancreatic calcifications may be noted.
Ultrasound can be used as a screening test. If overlying gas shadows secondary to bowel distention are present, it may not be specific.
CT scan is the most reliable imaging modality in the diagnosis of acute pancreatitis. The criteria for diagnosis are divided by Balthazar and colleagues into 5 grades, as follows:
Grade A – Normal pancreas
Grade B – Focal or diffuse gland enlargement
Grade C – Intrinsic gland abnormality recognized by haziness on the scan
Grade D – Single ill-defined collection or phlegmon
Grade E – Two or more ill-defined collections or the presence of gas in or nearby the pancreas
49. Acute and chronic haemorrhage, anemia.
Acute Blood Loss
- The effects of acute blood loss are mainly due to the loss of intravascular volume, which if massive can lead to cardiovascular collapse, shock, and death.
- The clinical features depend on the rate of hemorrhage and whether the bleeding is external or internal.
- If the patient survives, the blood volume is rapidly restored by the intravascular shift of water from the interstitial fluid compartment. This fluid shift results in hemodilution and a lowering of the hematocrit.
- The reduction in oxygenation triggers increased secretion of erythropoietin from the kidney, which stimulates the proliferation of committed erythroid progenitors (CFU-E) in the marrow
- It takes about 5 days for the progeny of these CFU-Es to mature and appear as newly released red cells (reticulocytes) in the peripheral blood.
- The iron in hemoglobin is recaptured if red cells extravasate into tissues, whereas bleeding into the gut or out of the body leads to iron loss and possible iron deficiency, which can hamper the restoration of normal red cell counts.
- Significant bleeding results in predictable changes in the blood involving not only red cells, but also white cells and platelets.
- If the bleeding is sufficiently massive to cause a decrease in blood pressure, the compensatory release of adrenergic hormones mobilizes granulocytes from the
intravascular marginal pool and results in leukocytosis
Chronic Blood Loss
- Chronic blood loss induces anemia only when the rate of loss exceeds the regenerative capacity of the marrow or when iron reserves are depleted and iron deficiency anemia appears
Anemias
- Anemia is defined as a reduction of the total circulating red cell mass below normal limits.
- reduces the oxygen-carrying capacity the blood,leading to tissue hypoxia
- Patient Appears Pale. Weakness,malaise,and easy fatigability
- The lowered oxygen content of the circulating blood lead to dyspnea on mild exertion
- Hypoxia Can cause fatty change in liver,myocardium,and kidney
-Adult men: Blood hemoglobin concentration <130g/L or hematocrit <39%
-Adult women: Blood hemoglobin concentration<120g/L or hematocrit <37%
Signs and symptoms
Recognized by abnormal results on screening laboratory tests. Symptoms vary depending on the level of anemia and time course.
Mechanisms causing anemia:
- Marrow production defects: hyperproliferation
- Erythrocyte maturation defects: ineffective erythropoiesis
- Decreased erythrocyte survival: blood loss or hemolysis
Acute anemia
Losses of 10-15% of total blood volume; hypotension and decreased organ perfusion
Loss of >30%; postural hypotension, tachycardia
Loss of >40% of blood volume; hypovolemic shock; confusion,dyspnea, diaphoresis
Chronic/Progressive anemia
Presentation depends on age of patient and adequacy of blood supply to organs Fatigue
Loss of stamina
Breathlessness
Pale skin and mucous membrane
Palmar crease lighter
Tachycardia
Forceful heartbeat
Strong peripheral pulses
Systolic murmur
Diagnosis
Do a complete blood count; erythrocyte count, erythrocyte indices, leukocyte count, platelet count, cell morphology, iron supply.
Iron deficiency in anemia
- chronic bleeding (hemoglobin contains iron) • excessive menstrual bleeding • non-menstrual bleeding • bleeding from the gastrointestinal tract (ulcers, hemorrhoids, etc.) • rarely, laryngological bleeding or from the respiratory tract
- inadequate intake (special diets low in dietary iron)
- substances (in diet or drugs) interfering with iron absorption
- malabsorption syndromes
- fever where it is adaptive to control bacterial infection
- blood donation
- Though genetic defects causing iron deficiency have been studied
- Mean corpuscular volume (MCV) is the average volume of a red blood cell. This is a calculated value derived from the hematocrit and red cell count. Normal range may fall between 80 to 100 femtoliters (a fraction of one millionth of a liter).
- Mean Corpuscular Hemoglobin (MCH) is the average amount of hemoglobin in the average red cell. This is a calculated value derived from the measurement of hemoglobin and the red cell count. Normal range is 27 to 32 picograms.
- Mean Corpuscular Hemoglobin Concentration (MCHC) is the average concentration of hemoglobin in a given volume of red cells. This is a calculated volume derived from the hemoglobin measurement and the hematocrit. Normal range is 32% to 36%.
- B12 deficiency can lead to anemia-B12 is essential for metabolism, formation of RBCs and maintaining CNS including brain and spinal cord
- Hemolytic anemia-due to hemolysis-abnormal breakdown of RBCs
- Hereditary anemia-defects in hemoglobin production, defects of RBC membrane production and defective red cell metabolism
- Thalassemia-abnormal form or inadequate amount of hemoglobin, large number of RBC are destroyed
- Sickle cell anemia-abnormally shaped red blood cells that cannot pass through blood vessels easily, they get stuck and block the flow of blood to limbs and organs.
Pernicious Anemia
Pernicious anemia is a specific form of megaloblastic anemia caused by an autoimmune
gastritis that impairs the production of intrinsic factor, which is required for vitamin B12 uptake from the gut. Iron Deficiency Anemia
- Caused by chronic bleeding or inadequate iron intake; results in insufficient
hemoglobin synthesis and hypochromic, microcytic red cells
Anemia of Chronic Disease
- Caused by inflammatory cytokines, which increase hepcidin levels and thereby sequester iron in macrophages, and also suppress erythropoietin production
Aplastic Anemia
- Caused by bone marrow failure (hypocellularity) due to diverse causes, including
exposures to toxins and radiation, idiosyncratic reactions to drugs and viruses, and
inherited defects in telomerase and DNA repair
Thalassemia Syndrome
The thalassemia syndromes are a heterogeneous group of disorders caused by inherited mutations that decrease the synthesis of either the α-globin or β-globin chains that compose adult hemoglobin, HbA (α2β2), leading to anemia, tissue hypoxia, and red cell hemolysis related to the imbalance in globin chain synthesis
β-Thalassemias
The β-thalassemias are caused by mutations that dimin- ish the synthesis of β-globin chains
Pathogenesis
Impaired β-globin synthesis results in anemia by two mechanisms. The deficit in HbA synthesis produces “under hemoglobinized” hypochromic, microcytic red cells with subnormal oxygen transport capacity. Even more important is the diminished survival of red cells and their precursors, which results from the imbalance in α- and β-globin synthesis.
α-Thalassemia
The α-thalassemias are caused by inherited deletions that result in reduced or absent synthesis of α- globin chains.
50. Disease manifestations of bones and joints. Methods of examinations
- Osteoporosis. One of the most prevalent bone conditions, osteoporosis involves bone loss, leading to weakened bones that are more likely to break. Osteoporosis is an invisible condition, often doing its damage without people realizing they have it
- Fracture. Acute fractures are usually due to trauma, although they can be related to bone cancer. Kids are more likely to have wrist fractures while breaking a fall during sports or at play. Older adults are more vulnerable to falls and hip injuries because of balance issues, and as their bones may be more fragile, are likelier to break their hips
- Bone cancer. Cancer that originates in the bone, called primary bone cancer, is rare, accounting for less than 1% of all new cancers diagnosed, according to the National Cancer Institute. Cancer that spreads to the bones from other parts of the body is more common, such as metastatic tumors from prostate or breast cancer. Multiple myeloma, a type of blood cancer, interferes with bone marrow function and new bone production in the hips, pelvis, ribs, shoulders and spine, increasing the risk of fracture
- Scoliosis. Abnormal, side-to-side curvature of the spine, resulting in an S- or C-shaped appearance when seen from behind, is called scoliosis. It’s commonly diagnosed in infants or children, but can persist into adulthood
- Osteoarthritis. The most common type, osteoarthritis is the “wear-and-tear” form that increases with age. Cartilage that normally cushions the joint breaks down over time, leading to stiffness and pain, especially with movement. With hip arthritis and knee arthritis, walking becomes more difficult as pain builds and flexibility decreases. Adults in their 50s and older are more likely to develop this chronic, progressive disease, and women are more vulnerable.
- Rheumatoid arthritis. Rheumatoid arthritis is an autoimmune condition affect the lining of the joints. As the immune cells interact with the local joint cells, he explains, it causes ever-increasing inflammation, with eventual damage and destruction of cartilage and bone
- Lupus. This autoimmune condition affects various parts of the body, including the skin, internal organs, blood, brain, bones and joints. Inflammation caused by lupus can trigger arthritis, particularly in the hands, elbows, shoulders, knees and feet.
- Gout. This type of arthritis most often affects the joint connecting the big toe to the rest of the foot. In gout, excess uric acid – a waste product in the blood – forms crystals in the joints. Gout flare-ups, which are extremely painful, frequently strike in the middle of the night. Men are more likely to have gout, although women become more vulnerable after menopause
- Bursitis. Bursitis involves inflammation of the small, fluid-filled sacs called bursae that cushion the joints and surrounding tendons, muscles and bone. With bursitis, overuse or sudden injury of joints such as the hip, elbow and shoulder can lead to flare-ups. Bacterial infections can sometimes cause bursitis
METHODS OF EXAMINATION
- General x-ray, MRT, CT, ultrasound
- Bone density can be measured via special x-ray or ultrasound machines
- Bone scintigraphy
- Palpatation with percussion
51. Acute tracheobronchitis, acute bronchitis, bronchiolitis.
TRACHEOBRONCHITIS
- occurs when the trachea or bronchi become inflamed.
- usually due to a viral or bacterial infection, can also be due to irritants,i.e. cigarette smoke.
- Inflamed trachea and bronchi usually results in difficulty breathing and a severe cough.
- is usually acute, which means it only lasts for a few weeks.
- Term tracheobronchitis refers to the set of symptoms experienced, so it’s technically not contagious. However, if the symptoms are the result of a viral or bacterial infection, it could be contagious.
Common symptoms:
- severe cough, sore throat
- Fatigue, nasal congestion
- shortness of breath, wheezing
- Nausea, vomiting, cyanosis Etiology:
Diagnosis: usually based on clinical symptoms, nasal swabs – bacterial and viral isolation Treatment:
- Viral infection: relieving symptoms, condition will pass unaided. Well hydrated, pain medications and cough suppressants. Humidifiers may help to breathe more easily and loosen the mucus in their lungs.
- Bacterial infection: antibiotics may be needed to clear it. But all of the above methods can still be used to help relieve symptoms.
ACUTE BRONCHITIS
= is a self-limiting lower respiratory tract infection (RTI) characterized by inflammation of the bronchi. Etiology
- Viruses (> 90% of cases)
- Influenza A and B, Parainfluenza, Adenovirus, RSV, Rhinovirus, Coronavirus
- Bacteria
- Environmental etiologies
Clinical features
- Cough: for > 5 days and resolves in 2–3 weeks
◆ Sputum’Eb’4B5’1C’D$”(“G6’(“?(D*$%%&’$”’*,C(D-*1,’?01M0(“”(“’
- Runny nose and sore throat (likely symptoms of the preceding or simultaneous URI)
- Chest pain and dyspnea
- Headache, Malaise, Myalgias
- Fever (uncommon)
Diagnostics – clinical diagnosis
- Auscultatory findings ○ Wheezing
- Rhonchi
○ Coarse crackles
- Further workup is indicated if pneumonia is suspected
Treatment
- Rest and adequate hydration
- NSAIDs
- Antibiotics: generally not recommended!
➢ Possible indications: patient groups with increased risk of bacterial infection (e.g., smokers, the elderly, patients with lung disease) and patients with suspected differential diagnosis
❖ Antitussives, expectorants, and bronchodilators are generally not recommended, but may be considered under specific circumstances (e.g., wheezing in older children)
BRONCHIOLITIS
= is a lower respiratory tract infection (RTI) in which the bronchioles become inflamed because of a viral infection.
Epidemiology
- Primarily affects children < 2 years
- Peak incidence: 2–6 months of age
- Common during winter months
Etiology
- Respiratory syncytial virus (RSV) – main cause
- Less common: parainfluenza virus, influenza virus, adenovirus, rhinovirus, coronavirus, metapneumovirus
- Risk factors for severe disease:
- Prematurity
○ Congenital heart or lung disease
○ Neurologic disease
○ Immunodeficiency
Clinical features
- Initially presents with upper respiratory tract symptoms (e.g., rhinorrhea), fever, and cough
- Respiratory distress (usually occurs in infants)
- Tachypnea, prolonged expiration
○ Nasal flaring, intercostal retractions
○ Cyanosis
- Poor feeding in breastfed infants
- Auscultatory findings: wheezing, crackles Diagnostics – clinical diagnosis.
- Additional testing (not routinely done)
- Nasopharyngeal aspirate test for RSV
○ Chest x-ray: hyperinflation of the lungs, interstitial infiltrates, atelectasis
Treatment
- Supportive treatment (adequate hydration, relief of nasal congestion/obstruction, monitoring)
- Indications for hospitalization
- Toxic appearance, poor feeding, dehydration, lethargy
- Marked respiratory distress, oxygen saturation < 92%
- Age < 12 weeks and/or history of prematurity (< 34 weeks)
- Pre-existing heart, lung, or neurological conditions
- Immunodeficiency
- Bronchodilators, epinephrine, and corticosteroids have historically been part of the treatment for bronchiolitis, but recent guidelines no longer recommend them.
- Ribavirin (antiviral synthetic nucleoside analog): currently not recommended for routine treatment of bronchiolitis; may be considered in immunocompromised patients
Complications
- Respiratory failure and Pneumonia
Prevention
- Palivizumab : Short-acting monoclonal antibody that provides passive immunization to RSV infection. Indications: infants at risk for severe bronchiolitis (e.g., prematurity, heart or lung disease, immunocompromised states), Monthly IM administration during RSV season for the first year of life
52. Chronic bronchitis – etiology, pathogenesis, clinical presentation, types, diagnosis.
The chronic obstructive pulmonary diseases (COPDs) comprise emphysema and chronic bronchitis. Though it is possible to have emphysema without chronic bronchitis or the converse, most patients have some degree of both, though one may dominate the clinical scenario. They share common etiologies, the most significant of which is tobacco smoking. The term “chronic bronchitis” was used in previous definitions of COPD but is no longer included in the definition. The term is still used clinically. While both chronic bronchitis and emphysema are often associated with COPD, neither is needed to make the diagnosis. A Chinese consensus commented on symptomatic types of COPD that include chronic bronchitis and with frequent exacerbations
Chronic bronchitis is defined not morphologically but clinically as a persistent, productive (produces sputum) cough for at least three consecutive months in at least two consecutive years and without another identifiable cause. Chronic bronchitis is subdivided into three subtypes: simple chronic bronchitis, in which there is no PFT-based evidence of obstruction; obstructive chronic bronchitis, in which there is physiological evidence of obstruction; and chronic asthmatic bronchitis, in which a patient’s hyper-responsiveness to allergens or other stimuli contributes to the airway obstruction.
Etiology
There are many known causes of chronic bronchitis, but the most important causative factor is exposure to cigarette smoke either due to active smoking or passive inhalation. Many inhaled irritants to the respiratory tract such as smog, industrial pollutants, and toxic chemicals can cause chronic bronchitis. Although bacterial and viral infections usually cause acute bronchitis repeated exposure to infections can cause chronic bronchitis. The predominant viruses that are causative are Influenza type A and B, and the dominant bacterial agents are Staphylococcus, Streptococcus, and Mycoplasma pneumonia. People who have an associated background in respiratory diseases such as asthma, cystic fibrosis, or bronchiectasis have a higher predisposition to develop chronic bronchitis. People who have repeated exposure to environmental pollutants such as dust or airborne chemicals such as ammonia and sulfur dioxide have a higher risk of developing chronic bronchitis. Chronic gastroesophageal reflux is a well documented but less frequent cause of chronic bronchitis
Pathogenesis
Chronic bronchitis is a respiratory disease marked by overproduction of mucus and mucins. The excess mucus is produced by goblet cells and enlarged submucosal glands in response to longterm irritation. The mucous glands in the submucosa secrete more than the goblet cells. Mucins thicken mucus, and their concentration has been found to be high in cases of chronic bronchitis, and also to correlate with the severity of the disease. Excess mucus can narrow the airways, thereby limiting airflow and accelerating the decline in lung function, and result in COPD.
Excess mucus shows itself as a chronic productive cough and its severity and volume of sputum can fluctuate in periods of acute exacerbations. In COPD, those with the chronic bronchitic phenotype with associated chronic excess mucus, experience a worse quality of life than those without.
The increased secretions are initially cleared by coughing. The cough is often worse soon after awakening, and the sputum produced may have a yellow or green color and may be streaked with specks of blood. In the early stages, a cough can maintain mucus clearance. However, with continued excessive secretion, mucus clearance is impaired and when the airways become obstructed a cough becomes ineffective. Effective mucociliary clearance depends on airway hydration, ciliary beating, and the rates of mucin secretion. Each of these factors is impaired in chronic bronchitis. Chronic bronchitis can lead to a higher number of exacerbations and a faster decline in lung function.
Diagnosis
Diagnosis is suggested by history, physical examination, and chest imaging findings and is confirmed by pulmonary function tests.
53. Bronchial asthma – etiology, pathogenesis, clinical presentation, types, diagnosis.
Bronchial asthma: a chronic inflammatory disorder of the airways characterised by airway hypersensitivity and episodic attacks of airway narrowing; obstructive respiratory. Immune hyper reaction to specific allergens, exaggerated bronchospasm, SOB, wheezing.
- Triggered by various stimuli; dust, pollen, upper respiratory tract infection, cold air, exercise, smoke.
- Reversible, caused by narrowing of airways due to bronchospasm, inflammation and increased airway secretions.
- Inherited, environmental factors can increase likelihood of development
- Acute response; immediate bronchoconstriction on exposure to an inhaled antigen usually subsides within 90mins.
- Late phase response develops 3-5 hours after exposure to the trigger, it involves inflammation and increased airway responsiveness that prolongs the attack and causes a vicious cycle of exacerbations.
- Expiration prolonged, FEV1/FVC ratio below 70% decreased, hyperinflation of alveoli distal to obstructions increases in residual volume, increases work of breathing. Alveolar ventilation declines, mismatching of ventilation and perfusion occurs. Hypoxemia and hypercapnia. Pulmonary vascular resistance increases leading to rise of pulmonary artery pressure and increased load on the right side of the heart.
- CD4+, T-lymphocytes, eosinophils inflammation.
Pathogenesis:
Inhaled allergens and IgE from B cells form antigen-antibody complex, degranulate mast cells and constrict bronchi.
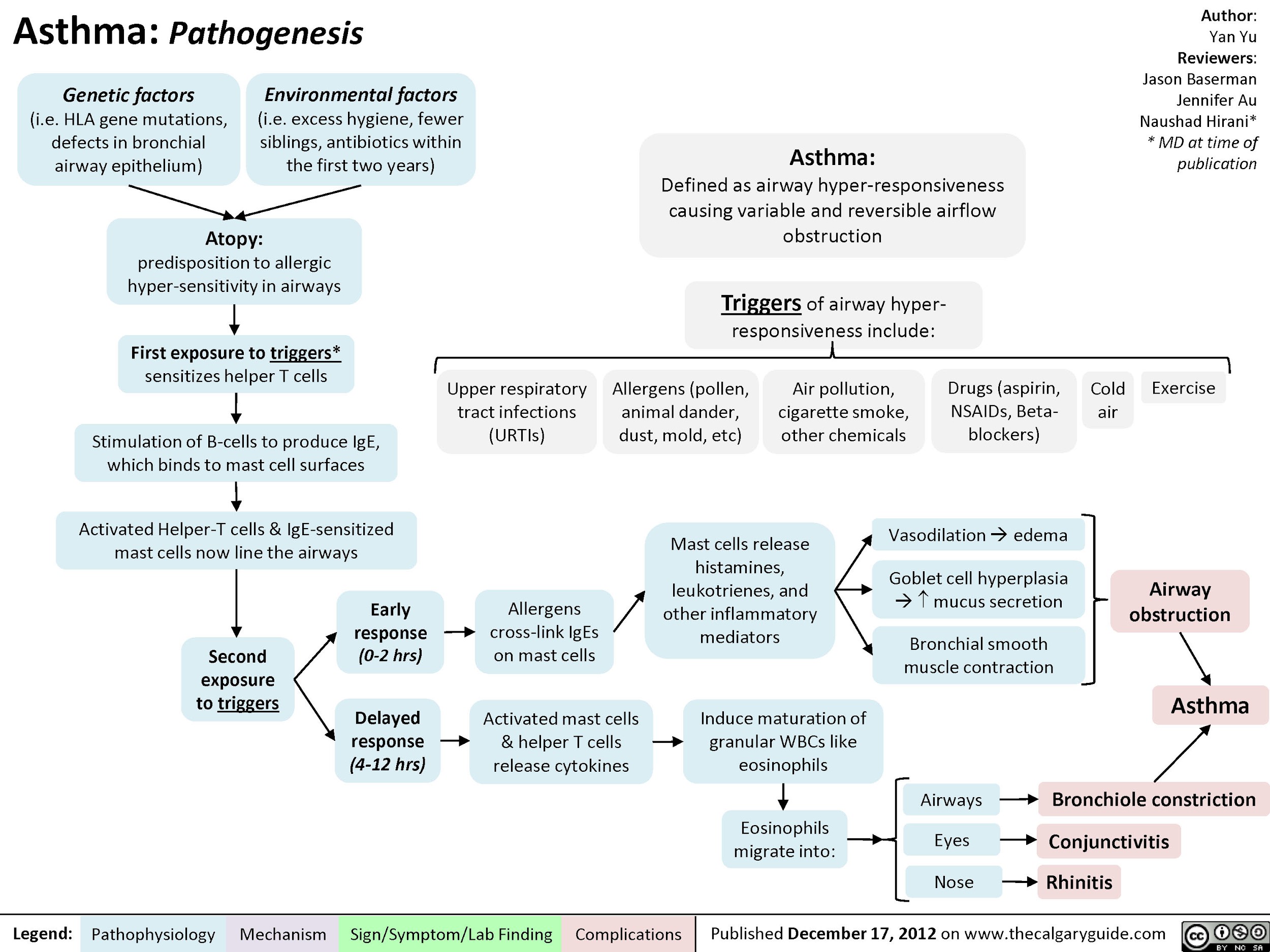
Diagnosed by: Bronchoprovocation test, Skin test for hypersensitivity.
Clinical presentation:
The characteristic symptoms of asthma are wheezing, dyspnea, and coughing, which are variable, both spontaneously and with therapy. Symptoms may be worse at night and patients typically awake in the early morning hours. Patients may report difficulty in filling their lungs with air. There is increased mucus production in some patients, with typically tenacious mucus that is difficult to expectorate. There may be increased ventilation and use of accessory muscles of ventilation. Prodromal symptoms may precede an attack, with itching under the chin, discomfort between the scapulae, or inexplicable fear (impending doom).
Typical physical signs are inspiratory, and to a greater extent expiratory, rhonchi throughout the chest, and there may be hyperinflation. Some patients, particularly children, may present with a predominant nonproductive cough (“cough-variant asthma”). There may be no abnormal physical findings when asthma is under control.
Types of Asthma:
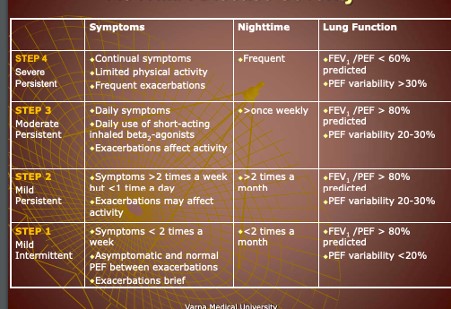
Diagnosis
Lung Function Tests
Simple spirometry confirms airflow limitation with a reduced FEV1, FEV1/FVC ratio,
Imaging
Chest roentgenography is usually normal but in more severe patients may show hyperinflated lungs. In exacerbations, there may be evidence of a pneumothorax. Lung shadowing usually indicates pneumonia or eosinophilic infiltrates in patients with bronchopulmonary aspergillosis (BPA). High-resolution CT may show areas of bronchiectasis in patients with severe asthma, and there may be thickening of the bronchial walls, but these changes are not diagnostic of asthma.
Skin Tests
Skin prick tests to common inhalant allergens (house dust mite, cat fur, grass pollen) are positive in allergic asthma and negative in intrinsic asthma, but are not helpful in diagnosis. Positive skin responses may be useful in persuading patients to undertake allergen avoidance measures.
54. Bronchiectatic disease – etiology, pathogenesis, clinical presentation, diagnosis.
Def: is a sac-like or cylindrical permanent dilation of the bronchi and bronchioles caused by destruction of the muscle and elastic supporting tissue as the result of a continuous cycle of infection and inflammation
ETIOLOGY
Any lung injury can cause bronchiectasis. There are two main categories of this condition. One is related to having cystic fibrosis (CF), and is known as CF bronchiectasis. CF is a genetic condition that causes an abnormal production of mucus.
The other category is non-CF bronchiectasis, which isn’t related to CF. The most common known conditions that can lead to non-CF bronchiectasis include:
- an abnormally functioning immune system
- inflammatory bowel disease
- autoimmune diseases
- chronic obstructive pulmonary disease (COPD)
- alpha 1-antitrypsin deficiency (an inheritable cause of COPD)
- HIV
- allergic aspergillosis (an allergic lung reaction to fungus)
- lung infections such as whooping cough and tuberculosis
PATHOGENESIS
- Mucus obstruction and chronic persistent infection are the etiology of bronchiectasis. Regardless of which may come first, both cause damage to the bronchial walls, leading to weakening and dilation
- On gross examination, bronchial dilation is classified as saccular, cylindrical, or varicose ● Can be congenital but is mostly acquired
CLINICAL PRESENTATION
- Clinically, most patients present with a long-standing history of either persistent or intermittent, sputum production
- Sputum could be mucoid, mucopurulent or viscous. Hemoptysis does occur and may range from minor, to life threatening
- Other symptoms include, constitutional symptoms such as fever, loss of appetite and shortness of breath
- Approximately 50% of patients have pleuritic chest pain, that may be due to peripheral bronchiectasis, or distal pneumonitis
- The clinical spectrum of the disease is broad. Some individuals with mild disease are completely asymptomatic between exacerbations. Others have chronic production of large amounts of mucoid sputum, that turns purulent, during infective episodes
- The most severely affected subjects usually have continuous purulent sputum production and a proportion of those with chronic symptoms, will have their disease progressing to chronic respiratory failure and will develop cor-pulmonale
DIAGNOSIS
Listen to lungs to check for abnormal sounds or evidence of airway blockage. A complete blood test is needed to look for infection and anemia. Other tests may include:
- sputum test to check your mucus for microorganisms such as viruses, fungi, or bacteria
- chest X-ray or CT scan to provide images of your lungs
- pulmonary function tests to find out how well air is flowing into your lungs
- QuantiFERON blood test or purified protein derivative (PPD) skin test to check for tuberculosis
- sweat test to screen for CF
55. Chronic obstructive pulmonary disease- etiology, pathogenesis, clinical presentation, diagnosis.
COPD is a lung disease characterised by persistent respiratory symptoms and airflow obstruction.
- It is a triad of emphysema, chronic bronchitis and small airway fibrosis.
- Chronic bronchitis is defined as a productive cough for at least 3 months in 2 consecutive years.
Risk Factors
- Tobacco smoking: associated with 80% of COPD cases
- Indoor air pollution: usually in developing world (cooking inside etc)
- Alpha-1 antitrypsin deficiency: an autosomal dominant condition which presents in younger patients (aged 20-40). It is a protease inhibitor with one of its actions being to prevent neutrophil elastase from breaking down alveolar structures. Therefore, a deficiency leads to the increased destruction of alveolar structures, resulting in earlyonset emphysema. Some cases of alpha-1 antitrypsin deficiency involve impaired secretion of alpha-1 antitrypsin by the liver, resulting in accumulation of it in the liver, and therefore cirrhosis.
History
- Presenting Complaint: COPD patients present with progressive dyspnoea and chronic productive cough.
- History of Presenting Complaint:
- Dyspnoea: initially exertional, but can progress to resting dyspnoea over the course of the condition (months to years).
- Chronic productive cough: usually colourless sputum, which may become green during lower respiratory tract infections (LRTIs)
●
●
| Recurrent LRTIs | |
| Fatigue | |
| Headache |
- (due to CO2 retention)
- Past Medical History
- Previous exacerbations or hospitalisations
- Medical comorbidities, including lung disease (such as asthma)
- Psychiatric comorbidities, including depression and anxiety
- Previous operations
- Medication/Allergies
- Regular medications (and any recent changes) *ACE-inhibitors can cause a dry cough
- Over-the-counter medications
- Allergies
- Family History
- Lung disease
- Liver disease (may suggest alpha-1 antitrypsin deficiency)
- Social History
- Smoking history: quantify in pack-years (1 pack-year = smoking 20 cigarettes a day for a year)
- Alcohol history
- Recreational drug use
- Occupation: may be exposed to indoor air pollution
Examination
A full respiratory examination should be performed in suspected cases of COPD.
- Most Common Findings
- Tachypnoea: due to an increased neural respiratory drive to breathe
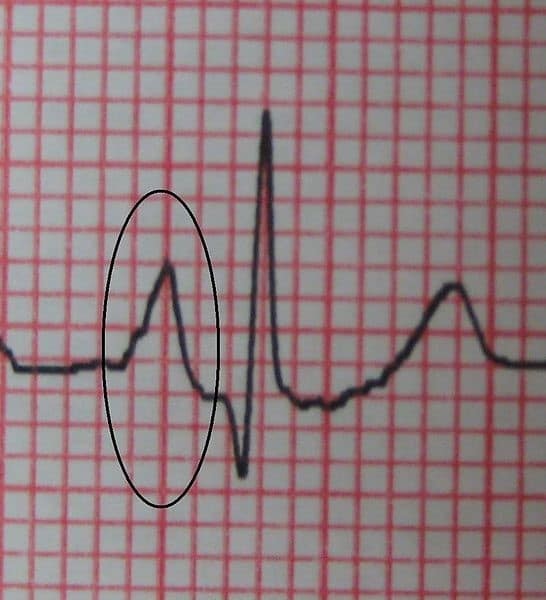 Wheeze on auscultation: due to inflammatory airway oedema and mucous obstructing the airway
Wheeze on auscultation: due to inflammatory airway oedema and mucous obstructing the airway- Pursed lips breathing: to increase airway resistance and therefore reduce expiratory flow limitation
- Less Common Findings
 Barrel chest : due to gas trapping
Barrel chest : due to gas trapping- Peripheral cyanosis
- Cor pulmonale (signs of right heart failure, such as peripheral oedema and hepatomegaly): due to pulmonary hypertension, which results from chronic hypoxic pulmonary vasoconstriction
- CO2 retention flap: while the exact mechanism is unknown, some hypothesise that it is due to abnormal function of the
diencephalon (which acts as a relay centre for sensory and motor impulses) Investigations Bedside:
Spirometry
- Typical finding in COPD: FEV1/FVC < 70%
- FEV1 is also used to classify the severity of COPD
Pulse oximetry
- Aim for SpO2 of 88-92%
- Avoid administering excessive amounts of O2:
- O2 displaces CO2 in haemoglobin, which increases CO2 in the blood
○ Increased CO2 in the blood cannot be removed due to failure of alveolar ventilation in emphysema, leading to hypercapnic respiratory failure Other investigations:
●: enables targeted antibiotic therapy during exacerbations of COPD
| Sputum culture | |
| ECG | : |
- cor pulmonale (peaked p waves and right axis deviation) Laboratory Investigations:
- Baseline blood tests: FBC, U&E, LFTs, CRP
- Arterial blood gas (ABG)
- During stable disease: PaCO2 >6.0 and bicarbonate >30 indicates that the patient is a “CO2-retainer”
○ During exacerbations: check for respiratory acidosis (PaCO2 >6.0 and pH
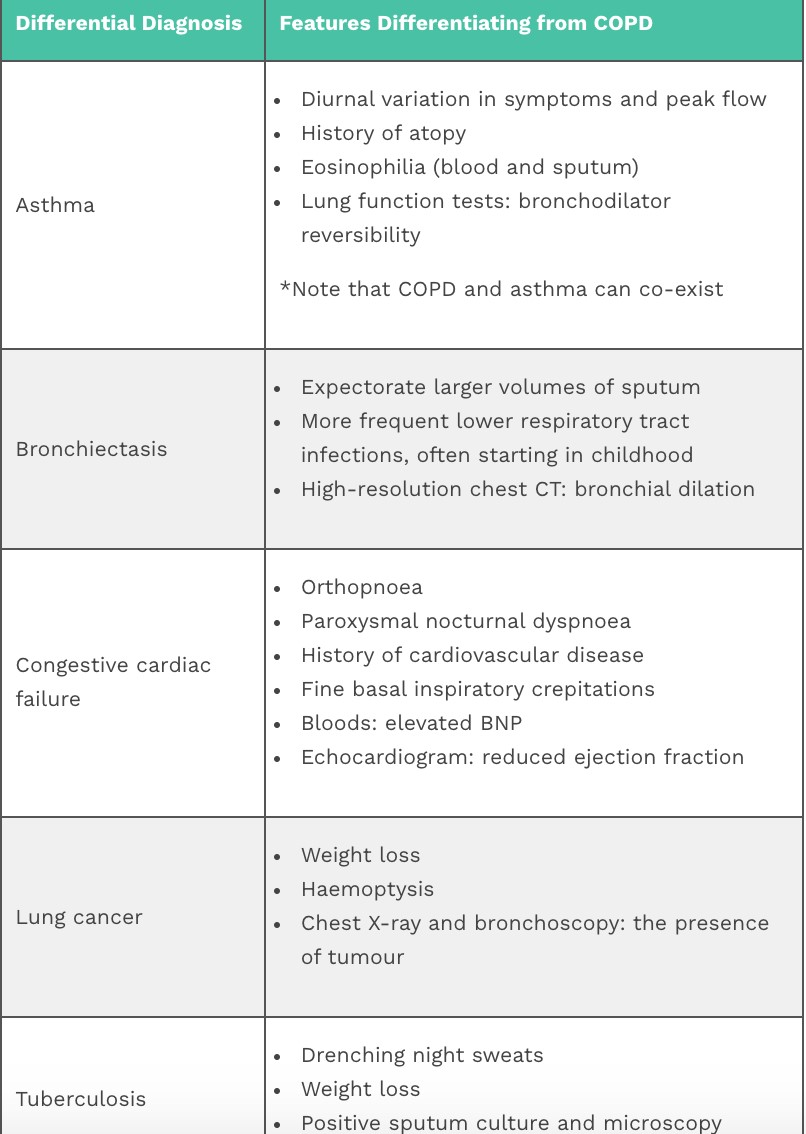

<7.35) Imaging:
- Chest X-ray:
hyperinflation10
-
- >6 anterior ribs or >10 posterior ribs visible in the midclavicular line
○ Flattened diaphragm ○ Hyperlucent lungs
Management (Long-Term)
- Conservative Management
- Smoking cessation
- Pulmonary rehabilitation
- Annual influenza vaccine and one-off pneumococcal vaccine
- Personalised self-management plan
- Medical Management: – Inhalers
– Long-Term Oxygen Therapy- Indications (one of the following):
○ SpO2 <88%
○ PaO2 <7.3kPa
- Contraindicated in current smokers due to the risk of explosion and/or burns
- Surgical Management
- Lung volume-reduction surgery: for very severe COPD, which does not respond to optimal medical management
- Lung transplantation: if not suitable for other surgical options
Complications
- Hypercapnic respiratory failure (PaO2 < 8.0 and PaCO2 > 6.0)
- Secondary polycythaemia (raised haemoglobin): due to chronic hypoxaemia
- Cor pulmonale: right heart failure, caused by pulmonary hypertension as a result of chronic hypoxic pulmonary vasoconstriction
- Bronchiectasis: due to chronic and repeated infections
- Anxiety and depression
- Osteoporosis: due to chronic steroid use, smoking, lack of bone-strength exercise and vitamin D deficiency ● Sleep disturbance
56. Pulmonary embolism – etiology, pathogenesis, clinical presentation, diagnosis
thrombi in the veins of the legs or pelvis (deep venous thrombosis)
Clots break off and pass through the veins and the right side of the heart before lodging in the pulmonary circulation infarction
Occasionally, blockages in the blood vessels are caused by substances other than blood clots, such as:
- Fat from the marrow of a broken long bone
- Collagen or other tissue
- Part of a tumor
- Air bubbles
Risk factors:
Recent surgery, especially abdominal/pelvic or hip/knee replacement; Thrombophilia; Leg fracture; Prolonged bed rest/reduced mobility; Malignancy; Pregnancy/postpartum; combined contraceptive pill, smoking, overweight.
Symptoms:
Small emboli may be asymptomatic, whereas large emboli are often fatal; Acute breathlessness, pleuritic chest pain, haemoptysis; dizziness; syncope; hypotension, tachycardia, tachypnea, fever; cyanosis
Other signs and symptoms that can occur with pulmonary embolism include:
- Leg pain or swelling, or both, usually in the calf
- Clammy or discoloured skin (cyanosis)
- Fever
- Excessive sweating
- Rapid or irregular heartbeat
- Lightheadedness or dizziness
●
In most cases a pulmonary infarction is caused by a blood clot that is relatively small, producing a fairly small infarction. In these cases, symptoms caused by the infarction itself may be very mild or nonexistent.
Larger pulmonary infarctions usually produce more severe symptoms, as do infarctions that affect the pleura (the fibrous membranes that protect and cover the lungs). These symptoms may include:
- hemoptysis (coughing or spitting up of blood)
- severe dyspnea (shortness of breath) • fever
- chest pain ( most typically, a pleurisy-like pain (chest pain that occurs when drawing a breath)
- (rarely) persistent hiccups
- lightheadedness
- weakness
Diagnosis:
patient history and risk factors; serum D-dimer testing for blood clots, arterial blood gas may show
low PaO2 and PaCO2; chest x-ray; ECG often shows tachycardia and various ST-T wave abnormalities
57. Pneumonia – etiology, pathogenesis, classification.
Pneumonia is an infection of the pulmonary parenchyma.
Classification and causes
- Community-acquired pneumonia: (CAP) May be primary or secondary to underlying disease. Typical organisms: Streptococcus pneumoniae (commonest), Haemophilus influenzae, Moraxella catarrhalis. Atypicals: Mycoplasma pneumoniae, Staphylococcus aureus, Legionella species, and Chlamydia. Gramnegative bacilli, Coxiella burnetii and anaerobes are rarer. Viruses account for up to 15%. Flu may be complicated by community-acquired MRSA pneumonia.
- Hospital-acquired: Defined as >48h after hospital admission. Most commonly Gram-negative enterobacteria or Staph. aureus. Also Pseudomonas, Klebsiella, Bacteroides, and Clostridia.
- Aspiration: Those with stroke, myasthenia, bulbar palsies, consciousness (eg post- ictal or intoxicated), oesophageal disease (achalasia, reflux), or poor dental hygiene risk aspirating oropharyngeal anaerobes.
- Immunocompromised patient: Strep. pneumoniae, H. influenzae, Staph. aureus,
M. catarrhalis, M. pneumoniae, Gram Ωve bacilli and Pneumocystis jirovecii (formerly named P. carinii, pp400–1). Other fungi, viruses (CMV, HSV), and mycobacteria.
Pathology
Classic pneumonia evolves through a series of pathologic changes. The initial phase is one of edema, with the presence of a proteinaceous exudate—and often of bacteria—in the alveoli. This phase is rarely evident in clinical or autopsy specimens because of the rapid transition to the red hepatization phase. The presence of erythrocytes in the cellular intra-alveolar exudate gives this second stage its name, but neutrophil influx is more important with regard to host defense. Bacteria are occasionally seen in pathologic specimens collected during this phase. In the third phase, gray hepatization, no new erythrocytes are extravasating, and those already present have been lysed and degraded. The neutrophil is the predominant cell, fibrin deposition is abundant, and bacteria have disappeared. This phase corresponds with successful containment of the infection and improvement in gas exchange. In the final phase, resolution, the macrophage reappears as the dominant cell type in the alveolar space, and the debris of neutrophils, bacteria, and fibrin has been cleared, as has the inflammatory response.
This pattern has been described best for lobar pneumococcal pneumonia and may not apply to pneumonia of all etiologies, especially viral or Pneumocystis pneumonia. In VAP, respiratory bronchiolitis may precede the development of a radiologically apparent infiltrate. Because of the microaspiration mechanism, a bronchopneumonia pattern is most common in nosocomial pneumonias, whereas a lobar pattern is more common in bacterial CAP. Despite the radiographic appearance, viral and Pneumocystis pneumonias represent alveolar rather than interstitial processes.
Classification
1- Anatomical classification:
- Lobar pneumonia-consolidation involves all or part of the lobe
- Bronchopneumonia- the consolidation involves scattered lobules
- Interstitial pneumonia- as in viral pneumonia where inflammatory infiltrate involve mainly interstitial tissue between alveoli
2- Etiological classification
The cause of pneumonia in patients is often difficult to determine because direct culture of lung tissue is invasive and rarely performed.
A- fungal
B-rickettsia- Coxiella burnetii, Rickettsia rickettsii
C-Mycobacterial
D-parasitic
E-non-infectious- aspiration of food, gastric acid, foreign body, aspiration of amniotic fluid
58. Lobar pneumonia – etiology, pathogenesis, pathomorphology, clinical picture, diagnosis.
Def: is the inflammation of one or several lobes of the lung, which is often caused by Streptococcus pneumonia
Etiology: Bacterial infection Pneumococcus (Streptoccous pneumonie). Other causative organisms that may cause a lobar pattern include Klebsiella pneumoniae, Legionella pneumophila, Haemophilus influenza, Mycobacterium tuberculosis
Pathogenesis: – The pathogens settle in the alveoli and cause a serous exudation – Thereby (dadurch) the surfactant synthese is disturbed and the pneumococci can penetrate the alveolar wall and can spread in one or several lung lobes
PATHOMORPHOLOGY
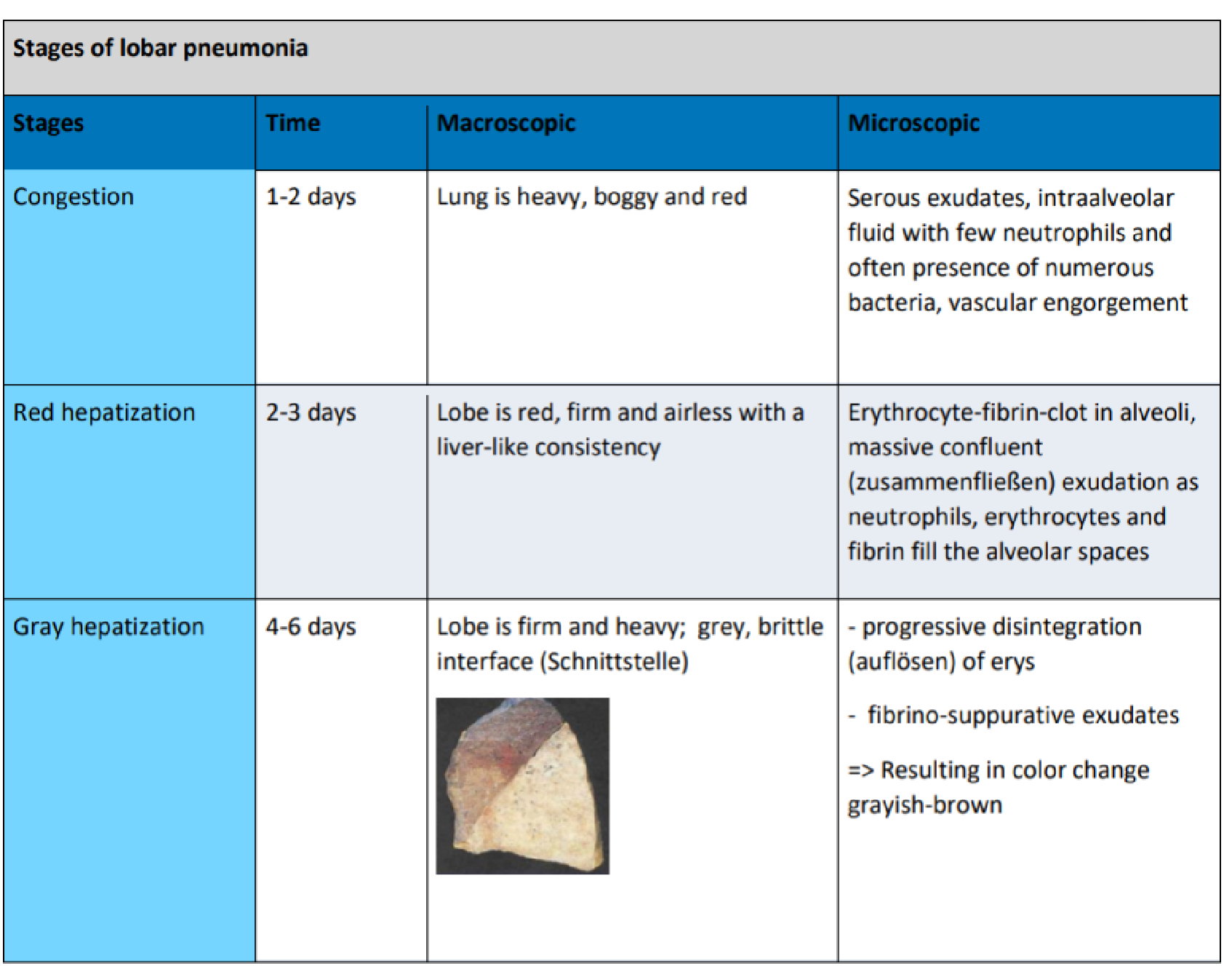
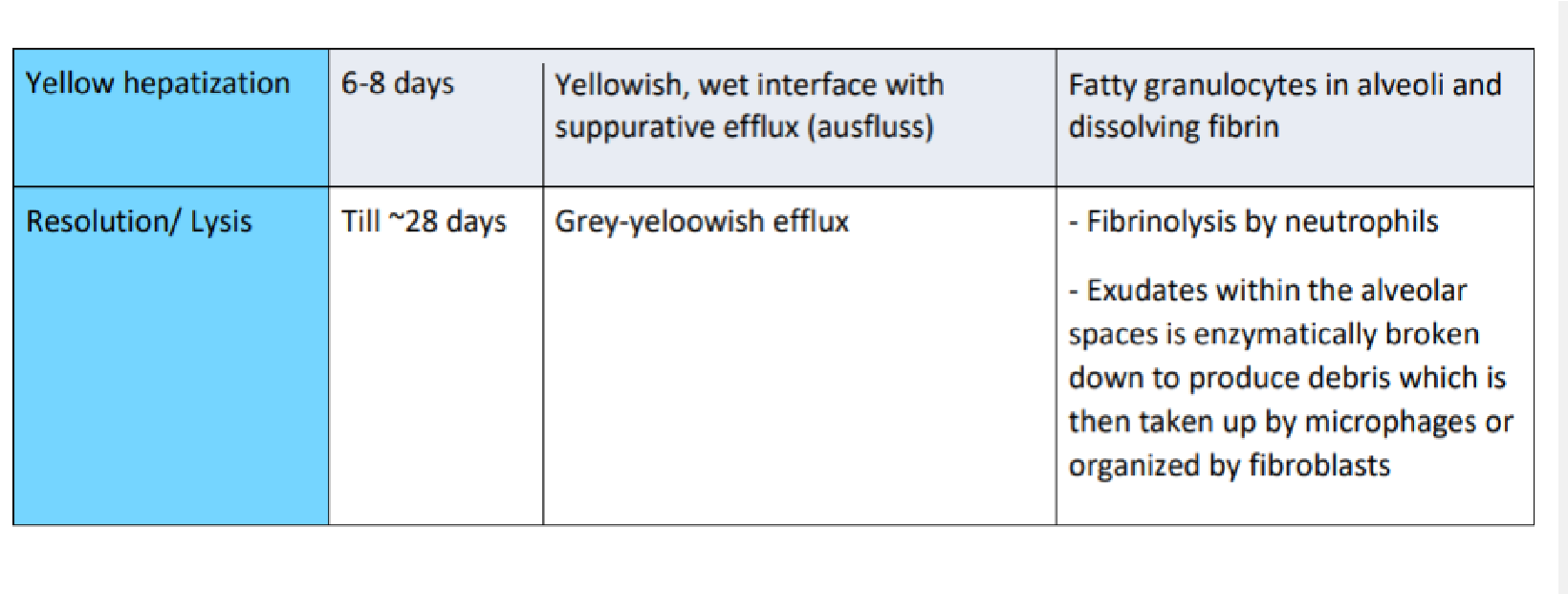
CLINICAL PICTURE
- productive cough
- Dyspnoea
- pyrexia/fever
- Rigours
- Malaise
- pleuritic pain
- Occasionally haemoptysis
Key features on physical examination are dullness in percussion in a lobar pattern, bronchial breathing, and adventitious breath sounds. A pleural rub and reduced expansion on the affected side may be present. Also increased vocal resonance.
When to hospitalise (point system)
Confusion
Urea>7mmol/L (Nitrogen>19)
Respiratory alkalosis (Resp. rate >30)
Blood pressure low <90/60
Or patients older than 65yrs old
0 points – can go home 1-2 points – hospitalisation
3+ points – urgent hospitalisation
DIAGNOSIS
- Radiograph
- CT
- Phsyical examination
- X-ray (m.pneumonia usually shows hilar consolidation)
- Lab
TREATMENT
Beta lactams – gram positive
Macrolides – for gram negative
Metronidazole – anaerobic organisms (if you suspect aspiration pneumonia)
59. Bronchopneumonia – etiology, pathogenesis, clinical presentation, diagnosis.
Bronchopneumonia is a form of pneumonia that affects both the alveoli in the lungs and the bronchi. Etiology:
- common cause of bronchopneumonia = bacterial lung infection – Streptococcus pneumoniae and Haemophilus influenza type b (Hib). Viral and fungal lung infections can also causes pneumonia.
- Pathogens enter the bronchi and alveoli and begin to multiply. The body’s immune system produces white blood cells that attack these germs, which causes inflammation. Symptoms often develop from this inflammation.
Risk factors for developing bronchopneumonia include:
- being under the age of 2 years, being over the age of 65 years
- smoking or excessive alcohol use, recent surgery or trauma
- recent respiratory infections, such as cold and the flu
- long-term lung diseases, such as COPD, cystic fibrosis, bronchiectasis, and asthma
- other health conditions, such as diabetes, heart failure, liver disease
- conditions that weaken the immune systems, such as HIV or certain autoimmune disorders
- taking drugs to suppress the immune system, such as for chemotherapy, organ transplantation, or long-term steroid use
Symptoms: vary, depending on the severity of the condition. May include: ● Fever, breathing difficulty, such as shortness of breath
- chest pain that may get worse with coughing or breathing deeply
- coughing up mucus
- Sweating, chills or shivering,nausea and vomiting, coughing up blood
- muscle aches, low energy and fatigue, loss of appetite, headaches
- confusion or disorientation, especially in older adults, dizziness Diagnosis: physical examination and medical history.
- Chest X-ray or CT scan: Bronchopneumonia will usually show up as multiple patchy areas of infection, usually in both lungs and mostly at the lung base. CT scan provides a more detailed look at the lung tissues.
- Blood tests: A high number of total white blood cells, along with high numbers of certain types of white blood cells, may indicate a bacterial infection.
- Bronchoscopy: This lighted instrument can take a closer look at the breathing tubes and take samples of lung tissue, while checking for infection and other lung conditions.
- Blood/Sputum culture. These tests show the type of organism causing the infection
- Pulse oximetry: This is a test used to calculate the amount of oxygen flowing through the bloodstream.
- Arterial blood gases. determine oxygen levels in a person’s blood.
Treatment:
- Viral bronchopneumonia – doesn’t require medical treatment unless severe. Improves on its own in two weeks.Viral infection like influenza, your doctor may prescribe antivirals to help reduce the length of your illness and the severity of your symptoms.
- Bacterial: antibiotics
- Hospital care: if infection is severe, and if you meet the risk factors Complications – esp if you are in the at risk group:
- Respiratory failure – require ventilator to assist with breathing
- Acute respiratory distress syndrome (ARDS). ARDS is a more severe form of respiratory failure and is life-threatening.
- Sepsis – the infection causes an exaggerated immune response that damages the body’s organs and tissues. Sepsis can cause multiple organ failure and is lifethreatening.
- Lung abscesses. These are pus-filled sacs that can form inside the lungs.
- Non-bacterial pneumonia-viral, mycoplasma pneumoniae, chlamydia pneumoniae.
Walking pneumonia or “atypical” pneumonia is a less severe form of bacterial pneumonia. Three specific infectious bacteria cause the majority of atypical pneumonia cases:
- Mycoplasma pneumoniae usually infects people under 40 with mild pneumonia symptoms. It commonly causes earaches, headaches, and a sore throat, as well.
- Chlamydophila pneumoniae is common in school-aged children and young adults.
- Legionella pneumophila is more severe, generally, and seen most often in older adults, people who smoke, and those with weakened immune systems. It is also called Legionnaires’ disease.
Several viruses can lead to viral pneumonia, including:
- adenoviruses, which can also cause the common cold and bronchitis
- chickenpox (Varicella zoster virus)
- flu (influenza viruses)
- respiratory syncytial virus, which causes cold-like symptoms
These viruses can be transmitted in communities, hospitals, and other healthcare settings.
- Lung cancer – etiology, pathogenesis, clinical presentation, diagnosis.
Disease which consists of uncontrolled cell growth in tissues of the lung. This growth may lead to metastasis, which is the invasion of adjacent tissue and infiltration beyond the lungs. The vast majority of primary lung cancers are carcinomas of the lung, derived from epithelial cells. Lung cancer, the most common cause of cancer-related death in men and women, is responsible for 1.3 million deaths worldwide annually.
There are two major types of lung cancer: • Non-small cell
• Small cell.
Non-small cell lung cancer (NSCLC) comes from epithelial cells (cells that line the airways and produce mucus, which lubricates and protects the lung) and is the most common type.
Small cell lung cancer begins in the nerve cells or hormone-producing cells of the lung. The term “small cell” refers to the size and shape of the cancer cells as seen under a microscope.
It is important for doctors to distinguish NSCLC from small cell lung cancer because the two types of cancer are usually treated in different ways.
Cigarette smoke contains over 60 known carcinogens, including radioisotopes from the radon decay sequence, nitrosamine, and benzopyrene. Additionally, nicotine appears to depress the immune response to malignant growths in exposed tissue Across the developed world, almost 90% of lung cancer deaths are caused by smoking.
Other risk factors genetic factors radon gas
asbestos and air pollution including secondhand smoke ionizing radiation, viral infections
Symptoms
Lung cancer begins in stealth mode. There are usually no symptoms or warning signs in the early stages. As it progresses, symptoms are typically non-specific and may include:
Persistent cough.
Chest pain, especially during deep breaths.
Wheezing or shortness of breath.
Coughing up bloody phlegm.
Fatigue.
cachexia (weight loss dysphonia (hoarse voice) clubbing of the fingernails (uncommon) dysphagia (difficulty swallowing) Fever (in pneumonia
Tumors in the top (apex) of the lung, known as Pancoast tumors,may invade the local part of the sympathetic nervous system, leading to changed sweating patterns and eye muscle problems (a combination known as Horner’s syndrome) as well as muscle weakness in the hands due to invasion of the brachial plexus.
Depending on the type of tumor, socalled paraneoplastic phenomena may initially attract attention to the disease. In lung cancer, these phenomena may include LambertEaton myasthenic syndrome (muscle weakness due to auto-antibodies), hypercalcemia, or syndrome of inappropriate antidiuretic hormone (SIADH)
Metastasis
Common sites of metastasis include the brain, bone, liver, contralateral (opposite) lung, pericardium, adrenal glands and kidneys. Superior and inferior vena cava syndrome
Pleural effusion
Bone pain and pathologic fractures
Central Nervous System – headache and vomiting
Diagnosis
Biopsy – the only way to make a diagnosis of lung cancer. A biopsy is the removal of a small amount of tissue for examination under a microscope.
Sputum cytology.
Bronchoscopy.
Needle aspiration
Bone marrow biopsy.
Thoracentesis. Thoracotomy. Thoracoscopy. Mediastinoscopy.
Non-small cell lung carcinoma (NSCLC) -80% earlier stages surgery • squamous cell lung carcinoma-in smokers • adenocarcinoma, in women and nonsmokers • large cell lung carcinoma. Non-small cell lung carcinoma (NSCLC) – 20% chemotherapy and radiotherapy
TNM Regional Lymph Node Classification System Supraclavicular zone (1) Superior
Mediastinal Nodes (2-4) Aortic Nodes (5-6) Inferior Mediastinal Nodes (7-9) Hilar, Interlobar, Lobar, Segmental and Subsegmental Nodes (10-14)
62. Abscess of the lung – etiology, pathogenesis, clinical presentation, diagnosis.
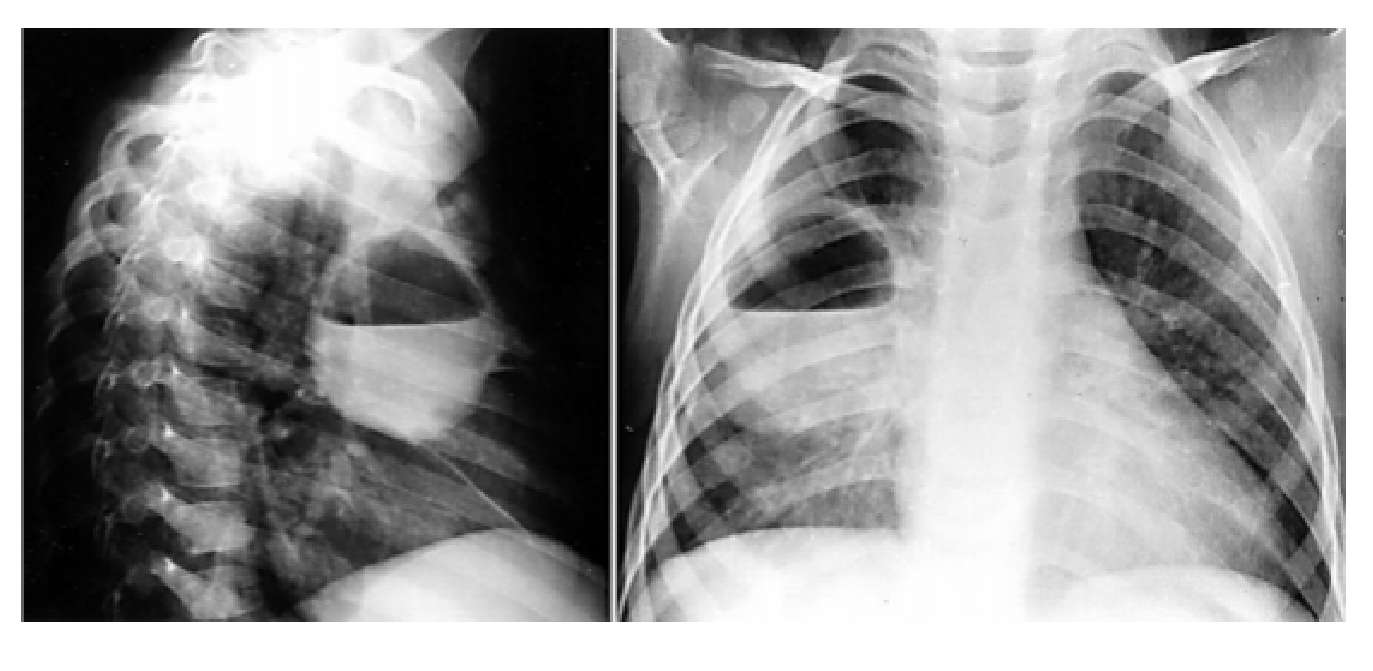
Lung abscess is a necrotising lung infection characterised by a pus filled cavitary lesion.
ETIOLOGY
- Poor oral health: People with gum disease are more likely to get an abscess.
- Your immune system isn’t working well: This can let in germs that aren’t usually found in your mouth or throat, like fungi or the bacteria that cause tuberculosis, strep throat, and
MRSA.
- Blocked airway: Mucus can form behind a tumor or foreign object in your windpipe and lead to an abscess. If bacteria get into the mucus, the blockage stops you from coughing it out.
- Blood-borne causes: It’s rare, but bacteria or infected blood clots from an infected part of your body can travel through your bloodstream and into your lung, where they cause an abscess.
PATHOGENESIS
● Anaerobic bacteria = peptostreptococcus, fusobacterium, prevotella, bacteroides ● Aerobic bacteria = streptococci, staphylococc
CLINICAL PRESENTATION
- Chest pain, especially when you breathe in
- Cough
- Fatigue
- Fever
- Loss of appetite
- Night sweats
- Sputum (a mixture of saliva and mucus) with pus that’s often sour-tasting, foul-smelling, or streaked with blood ● Weight loss
DIAGNOSIS
- Chest X-ray
- CT scan of the chest – shows air filled fluid level in the cavity
63. Lung tuberculosis – etiology, pathogenesis, clinical presentation, diagnosis.
TB = common infectious cause of morbidity and mortality worldwide that is caused by Mycobacterium tuberculosis and typically affects the lungs. Primary infection, which is transmitted via airborne droplets, is often initially asymptomatic. Typically, M. tuberculosis remains dormant as the host’s immune system keeps it in check (latent tuberculosis).
Epidemiology
- Sex: ♂ > ♀ (2:1)
- The incidence of multidrug-resistant tuberculosis is steadily rising Etiology
Risk factors
- Immunosuppression (TB is considered to be the most common cause of mortality in patients with HIV globally)
- Drug abuse, Alcoholism
- Malnutrition, Poverty
- Diabetes mellitus, Pre-existing damage to the lungs (e.g., silicosis, COPD)
- Residents and employees of congregate settings (e.g., prisons, hospitals, homeless shelters)
- Treatment with TNF-α inhibitors Pathophysiology:
- Alveolar macrophages (CD14+) phagocytose the TB bacteria but cannot eliminate them.
- Cord factor: a glycolipid in the cell wall of M. tuberculosis – inhibits fusion of phagosome + lysosome, = prevent lysis of phagocytosed mycobacteria
○ Hide inside macrophages = do not provoke a humoral immune response’*,’-/(’
/1″-’q’-/(0(C10(6’antibody detection tests play no role in the diagnosis of TB.The mycobacteria replicate safely within the macrophages
○ Phagocytosed M. tuberculosis can only be destroyed by activated T lymphocytes.
- Infection usually contained in the lung by formation of caseating granulomas – limit damage to the lungs and bacterial dissemination.
- Granuloma formation is caused by a delayed T cell-mediated reaction (i.e., type IV hypersensitivity reaction) that leads to the activation of alveolar macrophages (i.e., epithelioid cells) and their fusion into multinucleated giant cells.
○ The bacteria may remain dormant in the granulomas for many years without any active clinical disease manifesting (latent TB).
○ Immunosuppression (compromised T cell’C#,D-*1,G’q’+10=$,-’>$D-(0*$’>(D1=(’
$D-*)(6’0(?%*D$-(’*,’-/(’macrophages and spread into the lungs and other organs (active TB).
- IFN-γ deficiency: impaired phagocytosis and impaired granuloma’C10=$-*1,’q’+*””(=*,$-(+’ fX
Clinical features
- Latent infection: Asymptomatic and patient is not contagious.
- Active infection (either primary or reactivated)
- Constitutional symptoms: fever, weight loss, night sweats, fatigue, lymphadenopathy
○ Pulmonary symptoms: dyspnea, productive cough (possibly hemoptysis) lasting > 3 weeks
○ The patient is contagious
○ 80% pulmonary tuberculosis; 20% extrapulmonary tuberculosis
○ Common sites of extrapulmonary TB include the bones, pleura, lymphatic system, liver, CNS, heart, urogenital and gastrointestinal tracts, and the skin.
-
- Miliary tuberculosis: massive lymphohematogenous spread of Mycobacterium tuberculosis bacilli from a pulmonary or extrapulmonary focus with multiple organ involvement and very small granuloma lesions (1–2 mm)
- $DD1#,-“’C10’b’LB5’1C’$%%’(r-0$?#%=1,$0&’fX’D$”(“6’=$&’?0(“(,-’L‘4’ =1,-/”’$C-(0’*,*-*$%’*,C(D-*1,’10’&($0″’$C-(0
| Primary TB | Secondary TB |
| Definition | ●
● | Latent tuberculosis infection
(LTBI) ○ primary infection without any pathological findings on radiological imaging; however, screening tests indicating previous infection with M. tuberculosis are positive. ○ The lifetime risk of reactivation TB for a person with LTBI is about 5–10%. Active primary tuberculosis (only 1–5% of cases): primary infection with radiologicalpathological findings of tuberculosis | ●
● ● | following a latent primary TB infection; 80% of secondary infections begin in the lungs (many months or years may pass between the onset of primary and secondary infection).
Endogenous reactivation (very common) Exogenous reinfection (rare |
| Diagnosis | ●
● ● ● | Assess risk of active TB via history and physical examination
○ Moderate to high risk:’ D/(“-’r90$&’q’*C’”#MM(“-*)(’ 1C’?#%=1,$0&’fX6’sputum samples for culture, PCR’6’ $,+’=*D01″D1?&’q’*,*-*$-(’ -0($-=(,-’*C’fX’D1,C*0=(+’ E-/01#M/’D#%-#0(G’$,+’$%”1’ *C’PCR and microscopy are positive for tuberculous mycobacteria (while culture is pending) ○ Low risk: consider testing for latent tuberculosis Chest x-ray findings in tuberculosis ○ If reactivated disease: upper lobe cavitary lung lesions ○ If primary TB infection ■ Cavitation is uncommon in primary TB ■ Hilar lymphadenopathy ■ Pleural effusions ■ Ghon complex: sequelae of primary TB infection Sputum microscopy with acidfast stain (Ziehl-Neelsen stain) ○ Rapid results but lacks sensitivity ○ No differentiation between M. tuberculosis or nontuberculous mycobacteria possible Culture (gold standard) ○ Used for species identification, sensitivity testing, and to identify possibly resistances ○ Culturing can take up to six weeks (not useful for initial therapy planning) ○ E.g., Löwenstein–Jensen agar | ●
● ● ● | Test patients at risk for reactivation/new LTBI who’d benefit from treatment of LTBI.
○ Asymptomatic individuals w/ suspected new infection (e.g., close contacts of patient with active TB, health care workers) ○ People at risk for reactivation (e.g., immunocompromised patients) ^C’?$-*(,-“’.1#%+’>(,(C*-’C01=’ -0($-=(,-’q’TST or IGRA ○ d1″*-*)(’-(“-’q’s)$%#$-(’C10’ $D-*)(’fX’-1’+(D*+(’./(-/(0’ -0($-=(,-’C10’$D-*)(’10’latent TB is indicated. ○ Negative test ■ Repeat test after 8w in patients who are close contacts of patients with active TB/annually in patients with ongoing exposure (e.g., healthcare workers). ■ If none of the above applies, no repeat testing is necessary and the patient is considered negative for LTBI. Interferon-γ release assay (IGRA) ○ preferred in patients who received BCG vaccine. ○ ELISA test that measures the level of interferon-γ expressed by T cells after coming into contact with synthetic TB-specific peptides ○ Results within 24 hours Tuberculin skin test (TST) or purified protein derivative (PPD) test ○ TST is preferred for children younger than 5 ○ Only becomes positive 6–8 weeks after infection ○ Limited specificity’$,+’ “(,”*-*)*-&’Eb’7B5G |
| Treatment |
○ Monthly sputum samples for microscopy and culture ○ Monitor drug side effects: renal retention parameters, ophthalmological check-up , ENT, and liver function tests ACTIVE
LATENT
| |||
| Preventio n | BCG vaccine and test those at close contact |
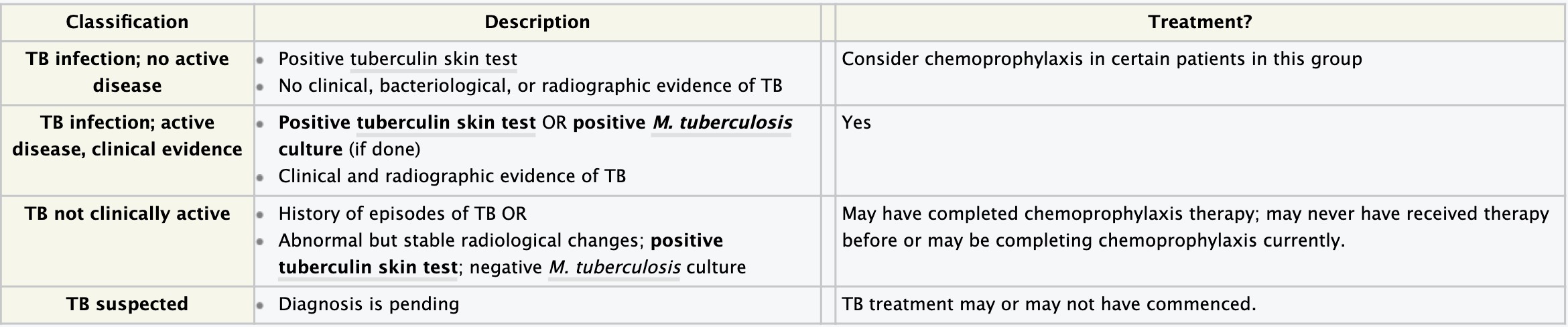
- Diseases of the pleura- pleurisy and hydrothorax
Pleurisy, also known as pleuritis, is inflammation of the membranes that surround the lungs and line the chest cavity (pleurae). This can result in a sharp chest pain while breathing. Occasionally the pain may be a constant dull ache. Other symptoms may include shortness of breath, cough, fever or weight loss, depending on the underlying cause.
Signs and symptoms
The defining symptom of pleurisy is a sudden sharp, stabbing, burning or dull pain in the right or left side of the chest during breathing, especially when one inhales and exhales. It feels worse with deep breathing, coughing, sneezing, or laughing. The pain may stay in one place, or it may spread to the shoulder or back. Sometimes, it becomes a fairly constant dull ache.
Depending on its cause, pleuritic chest pain may be accompanied by other symptoms.
- Dry cough
- Fever and chills
- Rapid, shallow breathing
- Shortness of breath
- Fast heart rate
- Sore throat followed by pain and swelling in the joints
Causes
- Viral infection (coxsackie B virus, HRSV, CMV, adenovirus, EBV, parainfluenza, influenza, COVID-19) is the most common cause of pleurisy.
- Aortic dissections
- Autoimmune disorders such as systemic lupus erythematosus (or drug-induced lupus erythematosus), Autoimmune hepatitis (AIH), rheumatoid arthritis and Behçet’s disease.
- Bacterial infections associated with pneumonia and tuberculosis
- Chest injuries (blunt or penetrating)
- Familial Mediterranean fever, an inherited condition that often causes fever and swelling in the abdomen or the lungs
- Fungal or parasitic infections
- Heart surgery, especially coronary-artery bypass grafting
- Cardiac problems (ischemia, pericarditis)
- Inflammatory bowel disease
- Lung cancer and lymphoma
- Other lung diseases like cystic fibrosis, sarcoidosis, asbestosis, lymphangioleiomyomatosis, and mesothelioma
- Pneumothorax
- Pulmonary embolisms, which are blood clots that enter the lungs
When the space between the pleurae starts to fill with fluid, as in pleural effusion, the chest pain can be eased but a shortness of breath can result, since the lungs need room to expand during breathing. Some cases of pleuritic chest pain are idiopathic, which means that the exact cause cannot be determined.
- Acute rheumatic fever- etiology, pathogenesis, pathomorphology, clinical presentation, forms diagnosis.
Acute rheumatic fever is a systemic disease of childhood, often recurrent that follows group A beta hemolytic streptococcal infection
It is a delayed non-suppurative sequelae to infection with GABH streptococci. Diffuse inflammatory disease of connective tissue, primarily involving heart, blood vessels, joints, soft tissue and CNS.
Diagrammatic structure of the group A beta hemolytic streptococcus Antigen of outer protein cell wall of GABHS induces antibody response in victim which result in auto immune damage to heart valves, subcutaneous tissue, tendons, joints & basal ganglia of brain
Pathogenesis
Delayed immune response to infection with group A beta hemolytic streptococci. After a latent period of 1-3 weeks antibody induced immunological damage occur to heart valves, joints, subcuta – neous tissue & basal ganglia of brain.
Pathomorphology
Fibrinoid degeneration of connective tissue, inflammatory edema, inflammatory cell infiltration & proliferation of specific cells resulting in formation of Aschoff nodules, resulting in: – Pancarditis in the heart – Arthritis in the joints – Aschoff nodules in the subcutaneous tissue, erythema marginatum -Basal ganglia lesions resulting in chorea
Clinical presentation
Flitting & fleeting migratory polyarthritis, involving major joints
Commonly involved joints-knee, ankle, elbow & wrist
Occur in 80%, involved joints are exquisitely tender
In children below 5 yrs arthritis usually mild but carditis more prominent
Arthritis do not progress to chronic disease
Tumor, dolor, calor, rubor, functio laesa
Erhytema marginatum
Occur in <5%
Transient, serpiginous -looking lesions of 1-2 inches in size
Pale center with red irregular margin
More on trunks & limbs & non-itchy
Worsens with application of heat
Often associated with chronic carditis
Subcutaneous
Rheumatic nodules
Occur in 10%
Painless, pea-sized, palpable nodules
Mainly over extensor surfaces of joints, spine, scapulae & scalp
Associated with strong seropositivity
Always associated with severe carditis
Carditis
Manifest as pancarditis (endocarditis, myocarditis and pericarditis), occur in 40- 50% of cases – the heart is enlarged heart sounds diminish in intensity with myocarditis new heart murmurs appear due to acute valvulitis.
Endocarditis and myocarditis go together as Rheumocarditis and pericarditis is only in 5%
Carditis is the only manifestation of rheumatic fever that leaves a sequelae & permanent damage to the organ
Valvulitis occur in acute phase
Chronic phase – fibrosis, sclerosis and calcification of heart valves
Histology
Fibrinoid necrosis and degeneration Aschoff bodies – rheumatic nodules Degenerated collagen surrounded by activated histiocytes and lymphoid cells
Diagnosis
Lab findings:
High ESR
Anemia, leukocytosis
Elevated C-reactive protien
ASO titre >200 Todd units. (Peak value attained at 3 weeks, then comes down to normal by 6 weeks) Anti- DNAse B test
Throat culture-GABH streptococci
Rheumatic fever is mainly a clinical diagnosis
No single diagnostic sign or specific laboratory test available for diagnosis Diagnosis based on MODIFIED JONES CRITERIA
66. Endocarditis – etiology, pathogenesis, clinical presentation, species diagnosis.
ETIOLOGY
Endocarditis is an infection of the endocardium, which is the inner lining of your heart chambers and heart valves. Most cases of endocarditis is due to a microbial infection of the endocardium. Endocarditis generally occurs when bacteria, fungi or other germs from another part of your body, such as your mouth, spread through your bloodstream and attach to damaged areas in your heart. If it’s not treated quickly, endocarditis can damage or destroy your heart valves and can lead to life-threatening complications. Treatments for endocarditis include antibiotics and, in certain cases, surgery
PATHOGENESIS
Any area of the heart that is exposed to turbulent blood flow (like a narrow cardiac valve or a septal defect) could be affected by endocarditis. Turbulence of blood flow causes damage to endocardial lining which exposes underlying collagen and tissue factor. This causes platelets and fibrin to adhere, forming a thrombosis (blood clot) – this is called non bacterial thrombotic endocarditis (NBTE) which occurs before bacteria shows up. Next is the microbial infection – microbe in the bloodstream. This might happen if a person has an open wound – dental/surgical procedure, injection with an infected needle etc.
Valves are most often affected (usually on the left side – mitral/aortic valves) because there is turbulent blood blow there.
RISK FACTORS
- Prosthetic valves
- Intravenous drug abuse
- Rheumatic heart disease – Congenital heart defects
CLINICAL PRESENTATION
- flu-like symptoms – these include having a temperature, tiredness, headaches, chills, a cough and sore throat
- unexplained weight loss
- pale skin
- aching muscles and joints
- heart murmurs (an abnormal heart sound)
SPECIES – The oral cavity, skin, and upper respiratory tract are the respective primary portals for viridans streptococci, staphylococci, and HACEK organisms (Haemophilus species, Aggregatibacter aphrophilus, A. actinomycetemcomitans, Cardiobacterium species, Eikenella species, and Kingella species). In addition to the usual causes of endocarditis, these cases can be due to Pseudomonas aeruginosa and Candida species, and sporadic cases can be caused by unusual organisms such as Bacillus, Lactobacillus, and Corynebacterium species.
DIAGNOSIS
- Blood tests to find out what type of bacteria is causing the inflammation.
- An echocardiogram (echo) to look for signs of damage in your heart.
- An electrocardiogram (ECG) to look for an abnormal heart rhythm.
- A chest X-ray to check for fluid build-up.
- An MRI scan to get a clearer image of your heart
67. Mitral insufficiency – etiology, pathomorphology, clinical presentation, diagnosis.
Also known as mitral regurgitation (MR) is the leakage of blood from the left ventricle into the left atrium due to incomplete closure of the mitral valve during systole.
Etiology
- Primary MR (organic): MR caused by direct involvement of the valve leaflets or chordae tendinae
- Degenerative mitral valve disease (mitral valve prolapse, mitral annular calcification, ruptured chordae tendinae)
○ Rheumatic fever
○ Infective endocarditis
○ Ischemic MR (e.g., papillary muscle rupture following acute MR)
- Secondary MR (functional): caused by changes of the LV that lead to valvular incompetence
- CAD or prior MI causing papillary muscle involvement
○ Dilated cardiomyopathy (e.g., peripartum cardiomyopathy) and left-sided heart failure
- Acute MR: Acute dysfunction of the mitral valve leads to volume overload and symptoms of acute heart failure.
- Chronic MR: To preserve cardiac output, valve dysfunction is initially compensated for by cardiac remodeling. Over time, remodeling affects LVEF, leading to heart failure
Pathophysiology
- Acute MR’q’V’O<’end-diastolic volume’’q’0$?*+’V’OY’$,+’?#%=1,$0&’?0(“”#0(’q’
?#%=1,$0&’)(,1#”’D1,M(“-*1,’q’pulmonary edema
- Chronic (compensated) MR: progressive dilation of the LV (via eccentric hypertrophyG’’q’ V’)1%#=(’D$?$D*-&’1C’-/(’O<’Epreload and afterload’0(-#0,’-1’,10=$%’)$%#(“G’q’V’(,+9 diastolic’)1%#=(’q’=$*,-$*,”’V’stroke volume (normal EF)
- Chronic (decompensated) MR: progressive LV enlargement and myocardial’+&”C#,D-*1,’q’
W’stroke’)1%#=(’q’V’(,+9systolic and end-diastolic’)1%#=(’q’V’O<’$,+’OY’?0(“”#0(’q’
?#%=1,$0&’D1,M(“-*1,6’?1″”*>%(’$D#-(’pulmonary edema, pulmonary hypertension, and right heart strain
| ACUTE | CHRONIC | |||
| Diagnostics |
○ Symptoms of left-sided heart failure ○ Signs and symptoms of pulmonary edema (e.g., bibasilar, fine, late inspiratory crackles) ○ Cardiogenic shock: poor peripheral perfusion, tachycardia, tachypnea, and hypotension ○ Palpitations
○ No murmur in severe regurgitation with LV systolic dysfunction or hypotension ○ Potentially: S3 heart sound | ●
● | ○
○ ○ ○ Au ○ ○ ○ ○ ○ | Signs and symptoms Dyspnea (inc. exertional dyspnea), dry cough
Fatigue Palpitations Symptoms of left-sided heart failure (potentially also symptoms of right-sided heart failure) scultation Lateral displacement of the apical impulse Quiet S1 heart sound S3 heart sound in advanced stages of disease S4 heart sound may be heard in functional MR. Holosystolic murmur (highpitched, blowing) ■ Radiates to the left axilla and heard best over the apex (5th intercostal space at the left midclavicular line) ■ Intensity can be increased by increasing preload (e.g., leg raise) or afterload (e.g., handgrip, squatting) due to increased regurgitation. |
| Treatment |
be managed with medical therapy (e.g., diuretics, nitrates, antihypertensive drugs).
| Management of chronic MR is guided by the symptoms and extent of heart failure and the cause of MR. Medical therapy should be initiated in all patients to optimize cardiac function but surgery is the definitive treatment option. | ||
| Complicatio ns |
| |||
| ECG | Findings are often nonspecific and include:
abnormalities
| ECG changes usually reflect cardiac remodeling.
of patients)
|
Diagnostics:
- Transthoracic echocardiography (TTE) is used to confirm the diagnosis and classify severity in patients with suspected MR.
- Check ECG and troponin in acute MR to rule out myocardial infarct.
- Consider additional diagnostics (e.g., coronary angiography, blood cultures) depending on patient stability and the suspected underlying condition.
- Echocardiography: Used to
○ Assess the valve apparatus
○ Assess the size and function of the left ventricle and atrium
○ Grade the MR as mild, moderate, or severe
○ Primary MR: (table)
○ Secondary MR: May include
- Normal valve anatomy but abnormal function
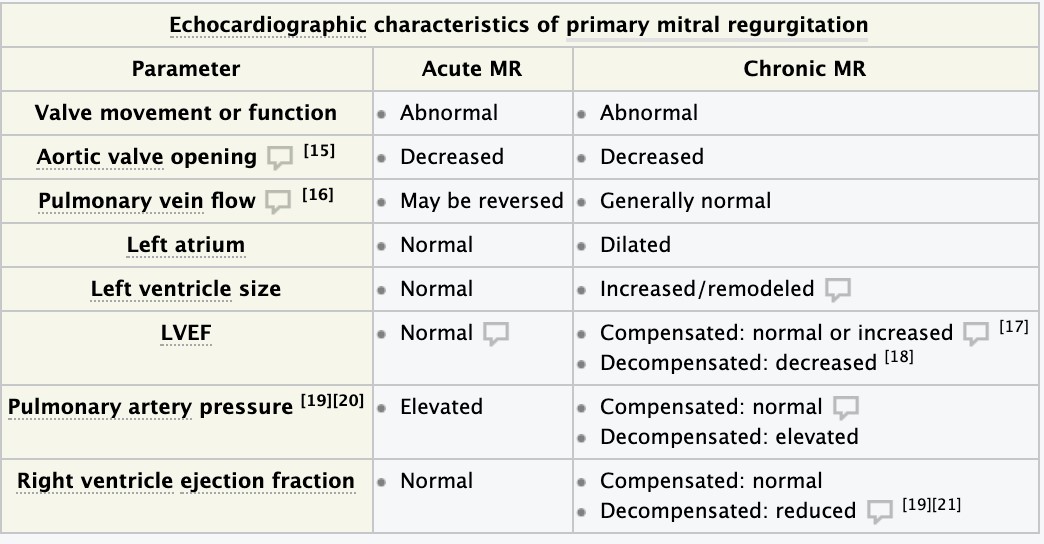 Signs of an underlying condition may be present (e.g., apical left ventricular ballooning in takotsubo cardiomyopathy)
Signs of an underlying condition may be present (e.g., apical left ventricular ballooning in takotsubo cardiomyopathy)
○ To assess for pulmonary edema
○ To rule out other causes of acute dyspnea
● Findings
○ Decompensated MR and acute MR: signs of pulmonary congestion
○ Acute MR: normal-sized cardiac silhouette
○ Chronic MR: Changes related to cardiac remodeling and associated heart failure may be visible.
■ LV enlargement: laterally displaced left cardiac border
■ LA enlargement: straightening of the left cardiac border and double density sign ■ Annular calcification may be visible as a C-shaped density.
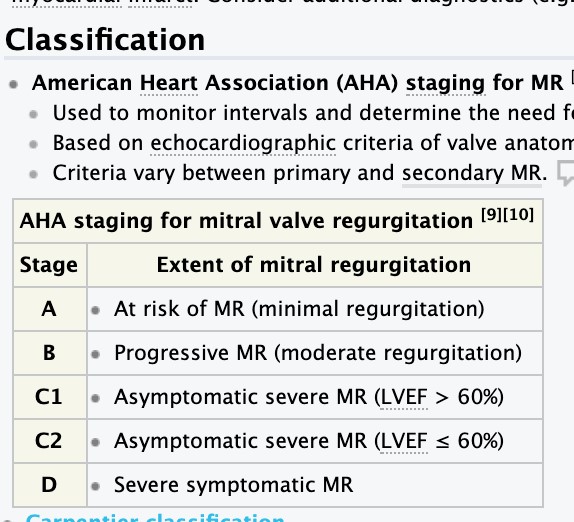
-68. Mitral stenosis – etiology, pathomorphology, clinical presentation, diagnosis
Mitral stenosis is a narrowing of the mitral valve opening that blocks (obstructs) blood flow from the left atrium to the left ventricle. Mitral stenosis usually results from rheumatic fever, but infants can be born with the condition. Mitral stenosis does not cause symptoms unless it is severe.
Etiology
- Most commonly due to rheumatic fever
- Autoimmune diseases: systemic lupus erythematosus, rheumatoid arthritis
- Congenital
- Some conditions may mimic mitral stenosis: bacterial endocarditis of the mitral valve with large vegetation, left atrial myxoma
- Degenerative aortic stenosis
The causes can be broadly classified as congenital, acquired, and rheumatic. Rheumatic MS usually follows recurrent attacks of rheumatic fever and is common in developing countries. Congenital MS is rare and is usually the result of chordal fusion, papillary muscle malposition/fusion (parachute mitral valve), or functional mitral stenosis (cor triatriatum). Rarely, acquired MS can be associated with systemic lupus erythematosus (SLE), rheumatoid arthritis, malignant carcinoid syndrome, Fabry disease, Whipple disease, drugs like methysergide, mitral annular calcification as seen in elderly patients, and end-stage renal disease.
Pathophysiology
- Mitral valve’”-(,1″*”’q’obstruction’1C’>%11+’C%1.’*,-1’-/(’%(C-’)(,-0*D%(’EO<G’q’%*=*-(+’+*$”-1%*D’
C*%%*,M’1C’-/(’O<’EW’(,+9+*$”-1%*D’O<’)1%#=(G’q’+(D0($”(+’”-018(’)1%#=(’q’+(D0($”(+’D$0+*$D’
1#-?#-’Eforward heart failure)
- j*-0$%’)$%)(’”-(,1″*”’q’*,D0($”(’*,’%(C-’$-0*$%’?0(“”#0(’q’>$D8#?’1C’>%11+’*,-1’%#,M”’q’*,D0($”(+’
?#%=1,$0&’D$?*%%$0&’?0(“”#0(’q’cardiogenic pulmonary edema’q’?#%=1,$0&’/&?(0-(,”*1,’q’ >$D8.$0+’/($0-’C$*%#0(’$,+’0*M/-’)(,-0*D#%$0’/&?(0-01?/&
Clinical features
- ^,*-*$%%&’$”&=?-1=$-*D’E1,”(-’b’KB’&($0″’$C-(0’$D#-(’0/(#=$-*D’D$0+*-*”G
- Dyspnea (paroxysmal nocturnal dyspnea) and orthopnea, especially when supine
- Hemoptysis
- Atrial fibrillation
- Later stages: signs and symptoms of right-sided heart failure
Diagnostics
- Auscultation (see auscultation in valvular defects)
- Diastolic murmur typically heard best at the 5th left intercostal space at the midclavicular line (the apex)
■ Heard loudest when the patient is lying on his/her left side.
○ Loud first heart sound (S1)
○ Opening snap of the mitral valve after S2: A high-frequency, early-to-mid diastolic sound that occurs when leaflet motion suddenly stops during diastole after the stenosed valve has reached its maximum opening
■ Shorter interval between S2 and opening snap indicative of more severe disease, because left atrial pressure is greater than left ventricular end diastolic pressure (LVEDP) ● Chest x-ray
○ Posterior-anterior image
■ LA enlargement’.
■ Signs of pulmonary congestion (see X-ray findings in pulmonary congestion)
○ Lateral image
■ Dorsal displacement of the esophagus (visible in barium swallow test)
■ Signs of right ventricular hypertrophy
- ECG
- P mitrale
○ Atrial fibrillation
○ Signs of right ventricular hypertrophy (Sokolow-Lyon index)
- Echocardiography: most important diagnostic method for detecting and assessing valvular abnormalities
- Abnormal valve mobility
○ Subvalvular thickening
○ Leaflet thickening
○ Calcification
- Coronary angiography may be conducted prior to surgical interventions to assess the associated risk of coronary artery disease
69. Aortic insufficiency – etiology, pathomorphology, clinical presentation, diagnosis.
Aortic insufficiency, also known as aortic regurgitation is the leaking of the aortic valve of the heart that causes blood to flow in the reverse direction during ventricular diastole, from the aorta into the left ventricle. This will result in the increased cardiac muscle function. Aortic valve fails to close properly, allowing backflow to the left ventricle during diastole.
Etiology
Rheumatic disease resulting in thickening, deformity and shortening of aortic valve cusps, changes that prevent proper opening during systole and closure during diastole. Infective Endocarditis can also result in perforation or erosion of one or more leaflets. Primary aortic root disease resulting in aortic annular dilation. Other causes include hypertension, trauma, failure of prosthetic valves.
Pathomorphology
This defect may result from conditions that cause scarring of the valve leaflets or from enlargement of the valve orifice to the extent that the valve leaflets no longer meet. – Acute aortic regurgitation is characterized by the presentation of a sudden, large regurgitant volume to a LV of normal size that has not had time to adapt to the volume overload.
- The heart responds with use of the Frank-Starling mechanisms and an increase in heart rate, these compensatory mechanisms fail to maintain the cardiac output. – As a result, there is severe elevation in left ventricular end-diastolic pressure, which is transmitted to the left atrium and pulmonary veins, culminating in pulmonary edema – A decrease in cardiac output leads to sympathetic stimulation and a resultant increase in heart rate and peripheral vascular resistance that cause the regurgitation to worsen. – Death from pulmonary edema, ventricular arrhythmias, or circulatory collapse is common in severe acute aortic regurgitation
- Chronic aortic regurgitation, which usually has a gradual onset, represents a condition of combined left ventricular volume and pressure overload.
- As the valve deformity increases, regurgitant flow into the LV increases, diastolic blood pressure falls, and the LV progressively enlarges.
- Hemodynamically, the increase in left ventricular volume results in the ejection of a large stroke volume that usually is adequate to maintain the forward cardiac output until late in the course of the disease.
- Most persons remain asymptomatic during this compensated phase, which may last decades.
The only sign for many years may be a soft systolic aortic murmur.
Clinical presentation
- pulse has a rapid rise and fall
- elevated systolic pressure (large stroke volume)
-low diastolic pressure (diastolic run off of blood back into the left ventricle)
- carotid pulsations in the neck,
- throbbing peripheral pulses, and a
- left ventricular impulse that causes the chest to move with each beat.
- As the disease progresses, signs and symptoms of left ventricular failure begin to appear. These include orthopnea, and dyspnea (Left sited heart failure)
- Fatigue and weakness, especially when you increase your activity level
- Shortness of breath with exercise or when you lie down
- Swollen ankles and feet
- Chest pain (angina), discomfort or tightness, often increasing during exercise
- Lightheadedness or fainting
- Irregular pulse (arrhythmia)
- Heart murmur
- Sensations of a rapid, fluttering heartbeat (palpitations)
Diagnosis
- Echocardiogram. Sound waves directed at your heart from a wandlike device (transducer) held on your chest produces video images of your heart in motion. This test can help doctors closely look at the condition of the aortic valve and the aorta. It can help doctors determine the cause and severity of your condition, and see if you have additional heart valve conditions.
- Electrocardiogram (ECG). In this test, wires (electrodes) attached to pads on your skin measure the electrical activity of your heart. An ECG can detect enlarged chambers of your heart, heart disease and abnormal heart rhythms.
- Chest X-ray. This enables your doctor to determine whether your heart is enlarged — a possible indicator of aortic valve regurgitation — or whether you have an enlarged aorta. It can also help doctors determine the condition of your lungs.
- Exercise tests or stress tests. Exercise tests help doctors see whether you have signs and symptoms of aortic valve disease during physical activity, and these tests can help determine the severity of your condition. If you are unable to exercise, medications that have similar effects as exercise on your heart may be used.
- Cardiac MRI. Using a magnetic field and radio waves, this test produces detailed pictures of your heart, including the aorta and aortic valve. This test may be used to determine the severity of your condition.
- Cardiac catheterization. This test isn’t often used to diagnose aortic valve regurgitation, but it may be used if other tests aren’t able to diagnose the condition or determine its severity. Doctors may also conduct cardiac catheterization prior to valve replacement surgery to see if there are obstructions in the coronary arteries, so they can be fixed at the time of the valve surgery.
In cardiac catheterization, a doctor threads a thin tube (catheter) through a
blood vessel in your arm or groin to an artery in your heart and injects dye through the catheter to make the artery visible on an X-ray. This provides your doctor with a detailed picture of your heart arteries and how your heart functions. It can also measure the pressure inside the heart chambers.
70. Aortic stenosis – etiology, pathophysiology, clinical presentation, diagnosis.
ETIOLOGY
In aortic valve stenosis, the aortic valve between the lower left heart chamber (left ventricle) and the main artery that delivers blood from the heart to the body (aorta) is narrowed (stenosis).
When the aortic valve is narrowed, the left ventricle has to work harder to pump a sufficient amount of blood into the aorta and onward to the rest of your body. This can cause the left ventricle to thicken and enlarge. Eventually the extra work of the heart can weaken the left ventricle and your heart overall, and it can ultimately lead to heart failure and other problems.
Aortic valve stenosis can occur due to many causes, including:
- Congenital heart defect
- calcium buildup on the valve – Rheumatic fever
PATHOPHYSIOLOGY
Aortic valve stenosis — or aortic stenosis — occurs when the heart’s aortic valve narrows. This narrowing prevents the valve from opening fully, which reduces or blocks blood flow from your heart into the main artery to your body (aorta) and onward to the rest of your body.
When the blood flow through the aortic valve is reduced or blocked, your heart needs to work harder to pump blood to your body. Eventually, this extra work limits the amount of blood it can pump, and this can cause symptoms as well as possibly weaken your heart muscle.
Your treatment depends on the severity of your condition. You may need surgery to repair or replace the valve. Left untreated, aortic valve stenosis can lead to serious heart problems.
CLINICAL PRESENTATION
Aortic valve stenosis ranges from mild to severe. Aortic valve stenosis signs and symptoms generally develop when narrowing of the valve is severe. Some people with aortic valve stenosis may not experience symptoms for many years. Signs and symptoms of aortic valve stenosis may include:
- Abnormal heart sound (heart murmur) heard through a stethoscope
- Chest pain (angina) or tightness with activity
- Feeling faint or dizzy or fainting with activity
- Shortness of breath, especially when you have been active
- Fatigue, especially during times of increased activity
- Heart palpitations — sensations of a rapid, fluttering heartbeat
- Not eating enough (mainly in children with aortic valve stenosis)
- Not gaining enough weight (mainly in children with aortic valve stenosis)
DIAGNOSIS
- Echocardiogram
- Electrocardiogram
- Exercise stress test – Cardiac catheterization
71. Myocarditis.
Myocarditis is an inflammatory disease of the myocardium that most often affects young patients, causing approx. 10% of sudden deaths in young adults.
Epidemiology
- 1–5% of viral infections are estimated to have cardiac involvement.
- tC-(,’1DD#0″’*,’&1#,M’?$-*(,-“’E$)(0$M(’$M(o’b’_B’&($0″G’
- In 10% of sudden deaths in young adults, myocarditis is diagnosed in the post-mortem examination. Etiology:
| Infectious | Noninfectious | |
| ●
○ ● ○ ○ ○ ○ ○ ● ● ● | Viral
Most commonly implicated: Coxsackie B1-B5, parvovirus B19, HHV-6, adenovirus, HCV, HIV, EBV, CMV, Echovirus, H1N1 influenza A Bacterial β-hemolytic Strep. group A (acute rheumatic fever) C.diphtheriae (diphtheria, diphtheria toxin) Borrelia burgdorferi (borreliosis) Mycobacterium (tuberculosis) Mycoplasma Fungal (candidiasis, aspergillosis) Protozoan (Chagas disease, caused by Trypanosoma cruzi, is a common pathogen in South America) Parasitic (trichinella, echinococcus) |
(e.g., Kawasaki disease)
○ Radiation therapy ○ Medication (e.g., sulfonamides), chemotherapy (e.g., anthracycline) ○ Alcohol, cocaine |
Clinical features
- Often asymptomatic, but may range from acute, fulminant cases to chronically active or persistent myocarditis
- Preceding (1–2 weeks) flulike symptoms (fever6’$0-/0$%M*$6’=&$%M*$6’#??(0’0(“?*0$-10&’ -0$D-’*,C(D-*1,”G’q’*,+*D$-(“’?1″”*>%(’)*0$%’D$#”(
- In infants and young children: poor feeding, irritability, respiratory distress, and failure to thrive
- Fatigue, weakness, dyspnea, nausea, vomiting
- Cardiac arrhythmias: often sinus tachycardia, ventricular extrasystoles with palpitations or syncope, heart block with bradyarrhythmia
- Chest pain: indicates pericardial involvement (perimyocarditis)
- Acute decompensated congestive heart failure with dilated cardiomyopathy
- Cardiogenic shock in fulminant cases
● Auscultation findings
○ Brief systolic murmurs
○ Heart failure’q’Rp’E$,+’R_G’M$%%1?”
○ Pericarditis’q’pericardial friction rub Diagnostics
ECG and laboratory tests conducted to support the diagnosis.If the diagnosis is unclear, a biopsy may be indicated to help determine treatment.
- ECG/24-hour Holter monitoring, myocarditis should be suspected if found:
- Sinus tachycardia
- Arrhythmias: atrial or ventricular ectopic beats, complex ventricular arrhythmia, atrial tachycardia
- Repolarization abnormalities
○ ST depression, negative T waves
○ Possible ST elevations’.*-/’$’D1,D$)(’$”D(,+*,M’R’.$)(’’q’*,+*D$-(“’ perimyocarditis
- Heart block: right bundle branch block, complete heart block, AV block
- Rule out myocardial infarction: loss of R wave and pathological Q wave specific to myocardial infarction, not found in myocarditis
- Pericardial effusion: low voltage (low R-wave with poor progression)
○ Ventricles: dilation, diffuse hypokinesia, reduced ejection fraction, impaired contractility, regional wall motion abnormalities
○ Pericardial effusion: localized or circumferential fluid surrounding the ventricles ○ Exclusion of other possible etiologies of heart failure (e.g., heart defects)
- Myocardial biopsy
- Via cardiac catheterization of the left heart and MRI-supported biopsy
○ Indications
■ New onset heart failure, severe arrhythmias, resistance to treatment
■ Only performed if previous diagnostics are inconclusive and a definitive diagnosis of myocarditis might influence treatment
○ Results
■ Possible detection of viral DNA/RNA
■ Immunohistochemical detection of inflammation (with lymphocytic infiltrates in a viral etiology)
Treatment
- Supportive therapy
○ Inpatient surveillance (cardiac monitoring, oxygen administration, management of fluid status)
○ Rest; avoid physical activity
○ Analgesic drugs if required
- Causative treatment
○ Antibiotic therapy for bacterial and Antimycotic therapy for fungal
- Treatment of complications
○ Congestive heart failure: (e.g., management of fluid accumulation with diuretics, beta blockers , ACE inhibitors)
○ Treatment of cardiac arrhythmias (e.g., amiodarone)
○ Heart transplantation
Complications
- Progression to dilated cardiomyopathy’Eb’K45’1C’D$”(“G
- Concurrent pericarditis (perimyocarditis) that may lead to cardiac tamponade
(associated with large pericardial effusions)
- Heart failure or sudden cardiac death: probably due to ventricular tachycardia or fibrillation
- Acute and/or persistent arrhythmias
- Atrioventricular block
Prognosis
- Viral myocarditis: Most adults make full recovery; but, progression to dilated cardiomyopathy may occur.
○ However, prognosis is very poor for infants (75% lethality rate!)
○ Lethality rate for children is 25% and another 25% may develop chronic heart failure complications
● Markers of poor prognosis
○ Poor ventricular function, left bundle-branch block, low ejection fraction
○ Persistent viral genome (in the myocardium)
○ Chronic inflammation
72. Pericarditis, pericardial adhesions – etiology, pathogenesis, clinical presentation, species diagnosis.
Pericarditis is inflammation of the pericardium that may be acute or chronic.
Acute pericarditis is most commonly caused by viral infection; however, a number of conditions can cause an inflammatory response in the pericardium. Acute inflammation typically manifests with fever, pleuritic chest pain, and a pericardial friction rub on auscultation. The diagnosis is established based on clinical findings, although diffuse ST segment elevations on ECG and imaging may support the diagnosis. Acute pericarditis is usually self-limited, lasting days to weeks, and is therefore managed symptomatically.
If pericarditis lasts longer than three months, it is described as chronic pericarditis. Chronic pericarditis may either be constructive or effusive-constrictive.
Constrictive pericarditis is characterized by thickening and rigidity of the pericardium, resulting in both backward and forward failure. Patients typically present with fatigue, jugular vein distention, peripheral edema, and a characteristic pericardial knock on auscultation, which is caused by a sudden stop in ventricular diastolic filling.
Effusive-constrictive pericarditis is characterized by a thickened pericardium with an effusion; this can lead to cardiac tamponade. It may manifest with symptoms similar to constrictive pericarditis, symptoms of pericardial effusion, or cardiac tamponade. In both constrictive and effusive-constrictive pericarditis, imaging is used to confirm the diagnosis. Management consists of treatment of heart failure (e.g., diuretics) and pericardiectomy.
| Perimyocarditis | : |
| Transient constrictive pericarditis: |
Acute pericarditis: inflammation of the pericardium that either occurs as an isolated process or with concurrent myocarditis (myopericarditis). condition predominantly affecting the myocardium with pericardial involvement constrictive pericarditis that lasts < 3 months Chronic
pericarditis: inflammation of the pericardium that lasts > 3 months
Constrictive pericarditis is characterized by compromised cardiac function caused by a thickened, rigid, and fibrous pericardium secondary to acute pericarditis.
Effusive-constrictive pericarditis: Pericardial effusion occurs in addition to a thickened pericardium, which can lead to tamponade.
Etiology
- Idiopathic
- Infectious
Most commonly viral (e.g., coxsackie B virus)
Bacterial (e.g., Staphylococcus spp., Streptococcus spp., or M. tuberculosis) Fungal Toxoplasmosi
- Myocardial infarction
Postinfarction fibrinous pericarditis: within 1–3 days as an immediate reaction
Dressler syndrome: weeks to months following an acute myocardial infarction
- Postoperative (postpericardiotomy syndrome): blunt or sharp trauma to the pericardium
- Uremia (e.g., due to acute or chronic renal failure)
- Radiation
- Neoplasm (e.g., Hodgkin lymphoma)
- Autoimmune connective tissue diseases (e.g., rheumatoid arthritis, systemic lupus, scleroderma)
Clinical features
Acute pericarditis
- Chest pain
- Pleuritic chest pain
- Acute, sharp retrosternal pain caused by inflammation of the parietal pleura
- Typically aggravated by coughing, swallowing, or deep inspiration
- Other causes of pleuritic chest pain include pulmonary embolism, myocardial infarction, and pneumothorax.
- Improves on sitting and leaning forward
- Can radiate to the neck and shoulders (most commonly to the left side)
- Pericardial friction rub: high-pitched scratching on auscultation
- Indicates friction between the visceral and parietal pericardial tissue
- Best heard over the left sternal border during expiration while the patient is sitting up and leaning forward
- Occurs in atrial and ventricular systole, as well as early diastole ● Present in 85% of patients with acute pericarditis.
- Pericardial effusion
- Faint heart sounds
- Ewart sign
- Low-grade intermittent fever, tachypnea, dyspnea, nonproductive cough
Chronic pericarditis
Constrictive pericarditis
- Symptoms of fluid overload (i.e., backward failure) ● l#M#%$0’)(*,’+*”-(,-*1,6’V’\#M#%$0’)(,1#”’?0(“”#0(
- Kussmaul sign
- Hepatic vein congestion: hepatomegaly, painful liver capsule distention, hepatojugular reflux
- Peripheral edema or anasarca, ascites with abdominal discomfort
- Symptoms of reduced cardiac output (i.e., forward failure)
- Fatigue, dyspnea on exertion
- Tachycardia
- Pericardial knock: sudden cessation of ventricular filling during early diastole that is heard best at the left sternal border
- d#%”#”’?$0$+1r#”o’W’>%11+’?0(“”#0(’$=?%*-#+(’>&’$-’%($”-’KB’==’SM’+#0*,M’+((?’ *,”?*0$-*1,
Effusive-constrictive pericarditis
Effusive-constrictive pericarditis is characterized by symptoms of chronic constrictive pericarditis, pericardial effusion, or a mixture of both.
- Smaller or slow-growing effusions: Patients may be asymptomatic.
- Large effusions or rapidly growing effusions: symptoms of cardiac tamponade
- Beck triad
- Dullness at the left base of the lung due to compression
Diagnosis
Acute pericarditis
The diagnosis is based on the presence of the following clinical findings and ECG abnormalities, which are not always present in all cases.
- Characteristic chest pain
- Pericardial rub
- ECG abnormalities
- Pericardial effusion
Serial ECGs may be needed to show abnormalities. The ECG in acute pericarditis may show abnormalities confined to ST and PR segments and T waves, usually in most leads. (ECG changes in lead aVR are generally in the opposite direction of other leads.) Unlike MI, acute pericarditis does not cause reciprocal depression in ST segments (except in leads aVR and V1), and there are no pathologic Q waves. ECG changes in pericarditis can occur in 4 stages although not all stages are present in all cases.
- Stage 1: ST segments show upward concave elevation; the PR segments may be depressed (see figure Acute pericarditis: Stage 1 ECG).
- Stage 2: ST segments return to baseline; T waves flatten.
- Stage 3: T waves are inverted throughout the ECG; T wave–inversion occurs after the ST segment has returned to baseline and thus differs from the pattern of acute ischemia or MI.
- Stage 4: T wave changes resolve.
Echocardiography in acute pericarditis typically shows an effusion, which helps confirm the diagnosis, except in patients with purely fibrinous acute pericarditis in whom echocardiography is often normal. Findings indicating myocardial involvement include new focal or diffuse left ventricular dysfunction.
Because the pain of pericarditis may resemble that of acute MI or pulmonary infarction, additional tests (eg, serum cardiac marker measurement, lung scan) may be required if the history and ECG findings are atypical for pericarditis. Troponin is often elevated in acute pericarditis due to epicardial inflammation, so it cannot discriminate between pericarditis, acute infarction, and pulmonary embolism. Very high levels of troponin may indicate myopericarditis. The CK-MB (creatine kinase muscle band isoenzyme) level, which is less sensitive than the troponin level, is usually normal in acute pericarditis unless myocarditis is also present.
73. Pulmonary heart disease – etiology, pathogenesis, clinical presentation and stage diagnosis.
Right ventricular hypertrophy and dilation – chronic cor pulmonale secondary to hypoxic pulmonary hypertension
Right sided heart failure – engorged neck veins, liver congestion and enlargement, peripheral edema. Cor pulmonale or right-sided heart failure is an enlargement of the right ventricle due to high blood pressure in the arteries of the lungs usually due to high blood pressure in the arteries of the lungs usually caused by chronic lung disease.
Echocardiography of cor pulmonale enlarged right ventricle and right atrium, inferior vena cava and hepatic veins, tricuspid regurgitation, dilated pulmonary arterial hypertension
Prognosis and complications of COPD
Respiratory failure to hypercapnic coma
Right sided heart failure to intractable peripheral edema
Circulatory failure to shock
Pulmonary thromboembolic disease to sudden death
Thromboembolic pulmonary hypertension
Causes
- Acute respiratory distress syndrome
- COPD
- Primary pulmonary hypertension
- Blood clots in lungs
- Kyphoscoliosis
- Interstitial lung disease
- Cystic fibrosis
- Sarcoidosis
- Obstructive sleep apnea
- Sickle cell anemia
- Bronchopulmonary dysplasia
Pathogenesis
pathophysiology of cor pulmonale is a result of increased right-sided filling pressures from pulmonary hypertension that is associated with diseases of the lung —> increased Afterload leads to structural alterations in the right ventricle (RV) including RV hypertrophy (RVH) which can be seen in chronic cor pulmonale.
• Acute cor pulmonale: pulmonary embolism (more common) and acute respiratory distress syndrome (ARDS). The underlying pathophysiology in a massive pulmonary embolism causing cor pulmonale is the sudden increase in pulmonary resistance.
Clinical presentation
The symptoms/signs of pulmonary heart disease (cor pulmonale) can be non-specific and depend on the stage of the disorder, and can include blood backing up into the systemic venous system, including the hepatic vein. As pulmonary heart disease progresses, most individuals will develop symptoms like:
- Shortness of breath
- Wheezing
- Cyanosis
- Ascites
- Jaundice
- Enlargement of the liver
- Raised jugular venous pressure (JVP)
- Third heart sound
- Intercostal recession
- Presence of abnormal heart sounds
Diagnosis
Investigations available to determine the cause of cor pulmonale include the following:
- Chest x-ray – right ventricular hypertrophy, right atrial dilatation, prominent pulmonary artery
- ECG – right ventricular hypertrophy, dysrhythmia, P pulmonale (characteristic peaked P wave)
- Thrombophilia screen- to detect chronic venous thromboembolism (proteins C and S, antithrombin III, homocysteine levels)
| ● | Doppler echocardiography (best initial test) |
○ Hypertrophy and/or dilation of the right heart ventricle
○ Dilation of the coronary sinus
○ Estimation of pulmonary arterial pressure
○ mPAP’T’LB’==SM’$-’0(“-
○ Pulmonary capillary wedge pressureo’T’K4’==SM’*,’PH due to left heart disease
○ In pre-capillary PH: pulmonary vascular resistance’T’p’e11+’#,*-“’HKI
| ● | Electrocardiography: right axis deviation due to right ventricular hypertrophy |
| ● | Chest x-ray |
○ Pronounced central pulmonary arteries
○ Right heart hypertrophy (prominent right heart border)
○ Signs of underlying cause (e.g., nodular opacities in interstitial lung disease, barrel chest in COPD)
Symptoms are subtle in the early stages of the disease and passive hepatic congestion can be seen in advanced stages.In advanced stages, passive hepatic congestion secondary to severe right ventricular failure may lead to anorexia, right upper quadrant abdominal discomfort, and jaundice. In addition, syncope with exertion, which may also be seen in severe disease, reflects a relative inability to increase cardiac output during exercise with a subsequent drop in the systemic arterial pressure.
Elevated pulmonary artery pressure can lead to elevated right atrial, peripheral venous, and capillary pressure. By increasing the hydrostatic gradient, it leads to transudation of fluid and accumulation of peripheral edema.
74. Arterial hypertension- etiology, pathogenesis, clinical presentation, stage diagnosis.
ETIOLOGY
Causes include:
- Unknown cause (idiopathic pulmonary arterial hypertension)
- A genetic mutation passed down through families (heritable pulmonary arterial hypertension)
- Use of some prescription diet drugs or illegal drugs such as methamphetamines — and other drugs
- Heart problems present at birth (congenital heart disease)
- Other conditions, such as connective tissue disorders (scleroderma, lupus, others), HIV infection or chronic liver disease (cirrhosis)
- Gender – Men are more likely to have high blood pressure than women
- Smoking – Those who smoke are at an increased risk of having high blood pressure
PATHOGENESIS
Pulmonary hypertension is a type of high blood pressure that affects the arteries in your lungs and the right side of your heart. In one form of pulmonary hypertension, called pulmonary arterial hypertension (PAH), blood vessels in your lungs are narrowed, blocked or destroyed. The damage slows blood flow through your lungs, and blood pressure in the lung arteries rises. Your heart must work harder to pump blood through your lungs. The extra effort eventually causes your heart muscle to become weak and fail. In some people, pulmonary hypertension slowly gets worse and can be lifethreatening. Although there’s no cure for some types of pulmonary hypertension, treatment can help reduce symptoms and improve your quality of life.
CLINICAL PRESENTATION
- Shortness of breath (dyspnea), initially while exercising and eventually while at rest
- Fatigue
- Dizziness or fainting spells (syncope)
- Chest pressure or pain
- Swelling (edema) in your ankles, legs and eventually in your abdomen (ascites)
- Bluish color to your lips and skin (cyanosis)
- Racing pulse or heart palpitations
STAGE DIAGNOSIS
- Normal: systolic less than 120 mm Hg and diastolic less than 80 mm Hg
- Elevated: systolic between 120-129 mm Hg and diastolic less than 80 mm Hg
- Stage 1: systolic between 130-139 mm Hg or diastolic between 80-89 mm Hg
- Stage 2: systolic at least 140 mm Hg or diastolic at least 90 mm Hg
- Atherosclerosis – etiology, clinical presentation, diagnosis.
= is the most common type of arteriosclerosis, or thickening and stiffening of the arterial wall.
Epidemiology
- Leading cause of vascular disease worldwide
- Sex: ♂ > ♀
Etiology
| Modifiable risk factors | ● Nonmodifiable risk factors | ||
| ○
○ ○ ○ ○ ○ ○ ○ ○ ○ | Smoking
Diabetes mellitus Arterial hypertension Dyslipidemia High homocysteine levels (homocystinuria) Obesity High fibrinogen levels Hyperphosphatemia Stress Increased alcohol consumption | ○
○ | Family history: cardiovascular events in first-degree relatives below the age of 55 (♂)/65 (♀)
YM(o’=$%(“’T’_4’&($0″6’C(=$%(“’T’44’ &($0″’E?1″-=(,1?$#”(G |
Pathogenesis of atherosclerosis
- Chronic stress on the endothelium
- Endothelial dysfunction, which leads to
○ Invasion of inflammatory cells (mainly monocytes and lymphocytes) through the disrupted endothelial barrier
○ Y+/(“*1,’1C’?%$-(%(-“’-1’-/(’+$=$M(+’)(“”(%’.$%%’q’?%$-(%(-“’0(%($”(’*,C%$==$-10&’
=(+*$-10″’E(:M:6’D&-18*,(“G’$,+’?%$-(%(-9+(0*)(+’M01.-/’C$D-10’Edgh[G
○ PDGF stimulates migration and proliferation of smooth muscle cells (SMC) in the tunica intima and mediates differentiation of fibroblasts into myofibroblasts 3. Inflammation of the vessel wall
- Macrophages and SMCs ingest cholesterol from oxidized LDL and transform into foam cells.
- Foam cells accumulate to form fatty streaks (early atherosclerotic lesions).
- O*?*+9%$+(,’=$D01?/$M(“’$,+’RjF”’?01+#D(’(r-0$D(%%#%$0’=$-0*r’E(:M:6’D1%%$M(,G’q’ +()(%1?=(,-’1C’$’C*>01#”’?%$u#(’E$-/(01=$G’
- ^,C%$==$-10&’D(%%”’*,’-/(’$-/(01=$’E(:M:6’=$D01?/$M(“G’”(D0(-(’=$-0*r’
=(-$%%1?01-(*,$”(“’q’.($8(,*,M’1C’-/(’C*>01#”’D$?’1C’-/(’?%$u#(’+#(’-1’-/(’>0($8+1.,’ 1C’(r-0$D(%%#%$0’=$-0*r’q’=*,10’”-0(“”’0#?-#0(“’-/(’C*>01#”’D$?
- Calcification of the intima (the amount and pattern of calcification affect the risk of complications)
- d%$u#(’0#?-#0(’’q’(r?1″#0(’1C’-/01=>1M(,*D’=$-(0*$%’E(:M:6’D1%%$M(,G’q’-/01=>#”’
C10=$-*1,’.*-/’)$”D#%$0’1DD%#”*1,’10’”?0($+*,M’1C’-/01=>1M(,*D’=$-(0*$%
| Common sites | Atherosclerotic diseases |
| (in order of increasing frequency)
arteries
arteries
|
|
Diagnosis
Complete medical history and physical exam. Tests:
- Cardiac catheterization: locate the narrowing, blockages, and other abnormalities of specific arteries.
- Doppler sonography: A special probe is used to direct sound waves into a blood vessel to evaluate blood flow. An audio receiver amplifies the sound of the blood moving through the vessel. Faintness or absence of sound may mean there is a blockage. This is used to identify narrowing of the blood vessels of the abdomen, neck, or legs.
- Blood pressure comparison: Comparing blood pressure measurements in the ankles and in the arms helps determine any constriction in blood flow. Significant differences may mean blood vessels are narrowed due to atherosclerosis.
- MUGA/radionuclide angiography: a nuclear scan to see how the heart wall moves and how much blood is expelled with each heartbeat, while the person is at rest.
- Thallium/myocardial perfusion scan: also nuclear scan given at rest or after exercise that may reveal areas of the heart muscle that are not getting enough blood.
- CT: discover any coronary calcification that may suggest a future heart problem.
Treatment:
Primary and secondary prevention of atherosclerosis
- Lifestyle modifications
○ Weight reduction
○ Dietary modification
○ Moderate aerobic exercise
○ Smoking cessation
○ Moderate consumption of alcohol (about 1–2 glasses of wine or beer per day) presumably has a protective effect.
- Medical treatment: Treat hypertension, diabetes and hyperlipidemia
- Coronary artery disease – chronic coronary syndromes .
Chronic coronary syndrome (CCS), can also be referred to as stable ischemic heart disease
(SIHD).Stable ischemic heart disease (SIHD) refers to patients with known or suspected SIHD who have no recent or acute changes in their symptomatic status, suggesting no active thrombotic process is underway.
- Coronary artery disease – acute coronary syndromes- etiology, pathogenesis, clinical presentation, forms diagnosis.

Acute coronary syndrome is given to three types of coronary artery diseases associated with sudden rupture of plaque inside the coronary artery. Unstable angina, Non-ST segment elevation myocardial infarction (NSTEMI) and ST segment elevation myocardial infarction (STEMI).
Etiology
Acute coronary syndrome usually results from the buildup of fatty deposits (plaques) in and on the walls of coronary arteries, the blood vessels delivering oxygen and nutrients to heart muscles.
When a plaque deposit ruptures or splits, a blood clot forms. This clot blocks the flow of blood to heart muscles.
When the supply of oxygen to cells is too low, cells of the heart muscles can die. The death of cells — resulting in damage to muscle tissues — is a heart attack (myocardial infarction).
Even when there is no cell death, the decrease in oxygen still results in heart muscles that don’t work the way they should. This change may be temporary or permanent.
When acute coronary syndrome doesn’t result in cell death, it is called unstable angina.
Pathogenesis
ACS is caused by an imbalance between myocardial oxygen supply and demand resulting from one or more of the following four processes that lead to thrombus formation: (1) disruption of an unstable coronary plaque due to plaque rupture, erosion, or a calcified protruding nodule that leads to intracoronary thrombus formation and an inflammatory response; (2) coronary arterial vasoconstriction; (3) gradual intraluminal narrowing; and (4) increased myocardial oxygen demand produced by conditions such as fever, tachycardia, and thyrotoxicosis in the presence of fixed epicardial coronary obstruction. While plaque rupture remains the most common etiology of coronary thrombosis, erosion of an intracoronary plaque is increasing in frequency, perhaps related to the above mentioned shifts in the underlying risk factors for ACS.
Clinical presentation
The signs and symptoms of acute coronary syndrome usually begin abruptly. They include:
- Chest pain (angina) or discomfort, often described as aching, pressure, tightness or burning
- Pain spreading from the chest to the shoulders, arms, upper abdomen, back, neck or jaw
- Nausea or vomiting
- Indigestion
- Shortness of breath (dyspnea)
- Sudden, heavy sweating (diaphoresis) ● Lightheadedness, dizziness or fainting
- Unusual or unexplained fatigue
- Feeling restless or apprehensive
Diagnosis
ECG within 10mins
Biomarkers
Troponin I or T are gold standard.
78. Coronary artery disease – acute coronary syndromes– clinical presentation, changes, diagnosis.
Coronary artery disease is the narrowing or blockage of the coronary arteries, usually caused by atherosclerosis. Atherosclerosis (sometimes called “hardening” or “clogging” of the arteries) is the buildup of cholesterol and fatty deposits (called plaques) on the inner walls of the arteries. These plaques can restrict blood flow to the heart muscle by physically clogging the artery or by causing abnormal artery tone and function.
Without an adequate blood supply, the heart becomes starved of oxygen and the vital nutrients it needs to work properly. This can cause chest pain called angina. If the blood supply to a portion of the heart muscle is cut off entirely, or if the energy demands of the heart become much greater than its blood supply, a heart attack (injury to the heart muscle) may occur.
PATHOGENESIS
Your coronary arteries are shaped like hollow tubes through which blood can flow freely. The muscular walls of the coronary arteries are normally smooth and elastic and are lined with a layer of cells called the endothelium. The endothelium provides a physical barrier between the blood stream and the coronary artery walls, while regulating the function of the artery by releasing chemical signals in response to various stimuli.
Coronary artery disease starts when you are very young. Before your teen years, the blood vessel walls begin to show streaks of fat. As you get older, the fat builds up, causing slight injury to your blood vessel walls. Other substances traveling through your blood stream, such as inflammatory cells, cellular waste products, proteins and calcium begin to stick to the vessel walls. The fat and other substances combine to form a material called plaque.
Over time, the inside of the arteries develop plaques of different sizes. Many of the plaque deposits are soft on the inside with a hard fibrous “cap” covering the outside. If the hard surface cracks or tears, the soft, fatty inside is exposed. Platelets (disc-shaped particles in the blood that aid clotting) come to the area, and blood clots form around the plaque. The endothelium can also become irritated and fail to function properly, causing the muscular artery to squeeze at inappropriate times. This causes the artery to narrow even more.
Sometimes, the blood clot breaks apart, and blood supply is restored. In other cases, the blood clot (coronary thrombus) may suddenly block the blood supply to the heart muscle (coronary occlusion), causing one of three serious conditions, called acute coronary syndromes.
ACUTE CORONARY SYNDROME
Acute Coronary Syndrome is a name given to three types of coronary artery disease that are associated with sudden rupture of plaque inside the coronary artery:
- Unstable angina
- Non-ST segment elevation myocardial infarction or heart attack (NSTEMI) ● ST segment elevation myocardial infarction or heart attack (STEMI).
The location of the blockage, the length of time that blood flow is blocked and the amount of damage that occurs determines the type of acute coronary syndrome.
Unstable angina
Unstable angina is a new symptom or a change from stable angina. The angina may occur more frequently, occur more easily at rest, feel more severe, or last longer. Although this angina can often be relieved with oral medications, it is unstable and may progress to a heart attack. Usually more intense medical treatment or a procedure is required. Unstable angina is an acute coronary syndrome and should be treated as a medical emergency.
Heart attack: Non-ST segment elevation myocardial infarction (NSTEMI)
This heart attack, or MI, may not cause changes on an electrocardiogram (ECG). However, chemical markers in the blood indicate that damage has occurred to the heart muscle. In NSTEMI, the blockage may be partial or temporary, and so the extent of the damage relatively small.
Heart attack: ST segment elevation myocardial infarction (STEMI)
This heart attack, or MI, is caused by an abrupt and prolonged blocked blood supply. It affects a large area of the heart muscle, and so causes changes on the ECG as well as in blood levels of key chemical markers.
All acute coronary syndromes require emergency evaluation and treatment.
CLINICAL PRESENTATION
- Chest pain (angina)
- Shortness of breath ● Heart attack
DIAGNOSIS
- Electrocardiograph tests
- Laboratory Tests: include a number of blood tests used to diagnose and monitor treatment for heart disease
- Invasive Testing, such as cardiac catheterization, involves inserting catheters into the blood vessels of the heart in order to get a closer look at the coronary arteries.
- Nuclear Imaging
- Ultrasound Tests – Echocardiogram
- Radiographic Tests
79. Acute diffuse glomerulonephritis – etiology, pathogenesis, pathomorphology, forms.
- Historically called the “nephritic syndrome.”
- Characterized by development, over days, of azotemia, hypertension, edema, hematuria, proteinuria, and sometimes oliguria.
- Salt and water retention are due to reduced glomerular filtration rate (GFR) and may result in circulatory congestion.
- Red blood cell (RBC) casts on urinalysis confirm diagnosis.
- Proteinuria is usually <3 g/d. Most forms of acute GN are mediated by humoral immune mechanisms.
- Clinical course depends on underlying lesion Etiology:
- Infectious diseases
- Poststreptococcal glomerulonephritis – most common
- Nonstreptococcal postinfectious glomerulonephritis
- Bacterial: infective endocarditis, “shunt nephritis,” sepsis, pneumococcal pneumonia, typhoid fever, secondary syphilis, meningococcemia
- Viral: hepatitis B, infectious mononucleosis, mumps, measles, varicella, vaccinia, echovirus, and coxsackievirus
- Parasitic: malaria, toxoplasmosis
- IgA dominant postinfectious glomerulonephritis—usually post staphylococcal
- Multisystem diseases: SLE, vasculitis, Henoch-Schönlein purpura, Goodpasture’s syndrome
- Primary glomerular diseases: mesangiocapillary glomerulonephritis, Berger’s disease (IgA nephropathy), “pure” mesangial proliferative glomerulonephritis
- Miscellaneous: Guillain-Barré syndrome, irradiation of Wilms’ tumor, self-administered diphtheria-pertussis-tetanus vaccine, serum sickness Pathogenesis:
- It is ultimately the result of the formation of immune complexes within the glomerular basement membrane along with activation of complement. However, it is not clear if immune complexes are “preformed” or develop “in situ”
- Whatever their origin, deposition of immune complexes initiates inflammation of glomeruli, thus precipitating subsequent pathogenesis of nephritic syndrome.
- The source of the antigen precipitating creation of immune complexes can be both from an exogenous infectious agent or from an endogenous antigen. The prototypical infectious agent which precipitates APGN is streptococci whereas endogenous immune complexes released during evolution of Systemic Lupus Erythematosus can act as a culprit.
| Acute Poststreptococcal GN | Postinfectious GN |
|
|
Clinical Consequences
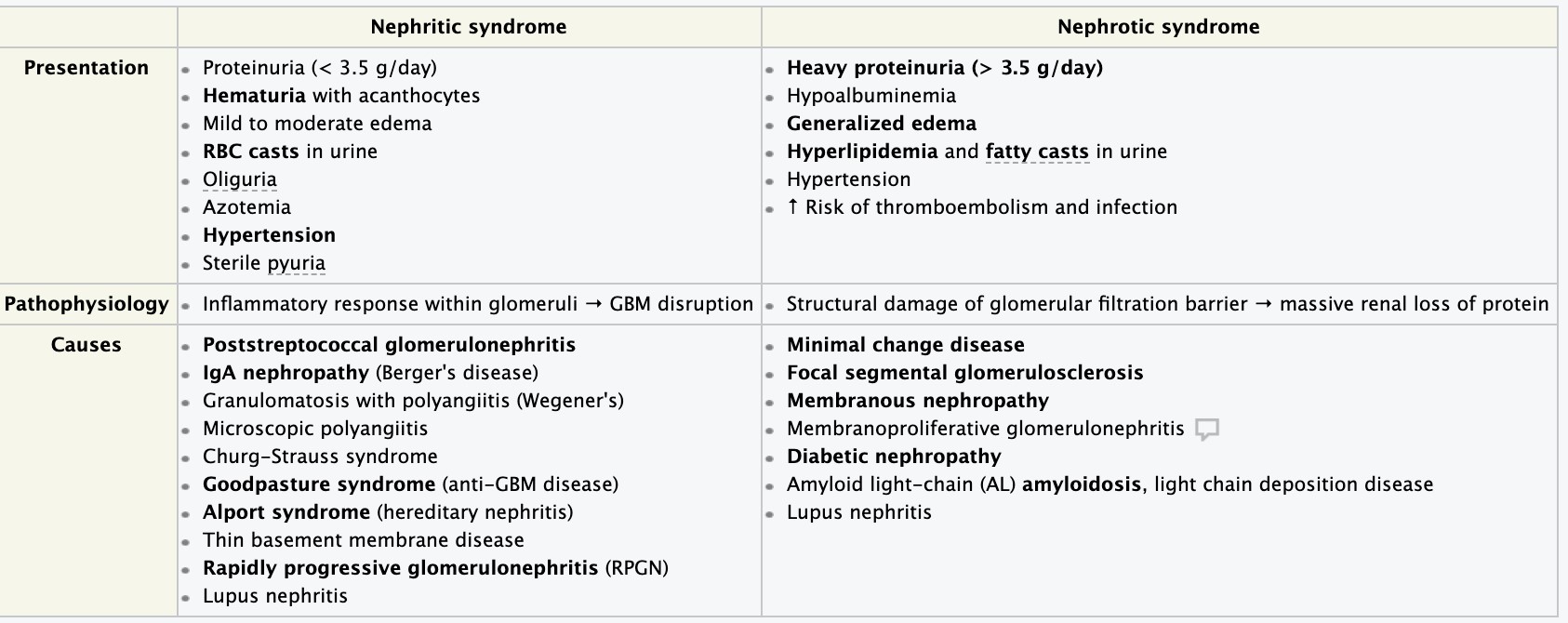 APGN typically presents with the signs of nephritic syndrome characterized by hematuria, pyuria, secondary hypertension, oliguria, and azotemia.
APGN typically presents with the signs of nephritic syndrome characterized by hematuria, pyuria, secondary hypertension, oliguria, and azotemia.- However, significant proteinuria reminiscent of nephrotic syndrome can also occur. constitutional symptoms are also frequently present.
- If severe, the disease can progress to the much more serious syndrome of rapidly progressive glomerulonephritis; however, most cases spontaneously resolve and prognosis is good.
80. Rapidly progressing (subacute) glomerulonephritis – etiology, pathogenesis, clinical presentation, diagnosis.
Rapidly progressive glomerulonephritis (RPGN) is a syndrome of the kidney that is characterized by a rapid loss of kidney function, (usually a 50% decline in the glomerular filtration rate (GFR) within 3 months) with glomerular crescent formation seen in at least 50% or 75% of glomeruli seen on kidney biopsies. Etiology
- In most cases immunological mediated
1’^-’*”’$’D%*,*D$%’”&,+01=(“q’,1-’$’”?(D*C*D’(-*1%1M*D$%’C10=’1C’h@ o Characterized by rapid loss of renal function, nephritic syndrome, severe oliguria 1’^C’#,-0($-(+’q0(,$%’C$*%#0(’*,’.((8″’10’=1,-/”
Pathogenesis
- Caused by number of different disease
§ 1. Anti-GBM antibody mediated crescentic GN (Goodpasture disease)
• Linear deposits of IgG and C3 in GBM
Q’^,’”1=(’?$-*(,-“’q$,-*9hXj’$,-*>1+*(“’>*,+’-1’?#%=1,$0&’$%)(1%$0’D$?*%%$0& >$”(=(,-’=(=>0$,(q’?01+#D(’D%*,*D$%’?*D-#0(’1C’?#%=1,$0&’/(=100/$M( associated with renal failure
Q’Y,-*9hXj’$,-*>1+*(“’*,’R(0#=’q+*$M,1″*”
Q’^=?10-$,-’-1’0(D1M,*c(’$,-*9hXj’$,-*>1+&9=(+*$-(+’D0(“D(,-*D’h@q’$CC(D-(+ individuals benefit from plasmapheresis
§ 2. Immune complex-mediated crescentic GN
Q’j$&’D1=?%*D$-(’$,&’1C’*==#,(’D1=?%(r’,(?/0*-*+(“q’*,D%#+*,M’?1”-“-0(?-1D1DD$%
GN, SLE, etc.
- Frequently shows cellular proliferation and influx of leukocytes within glomerular tuft in addition to crescent formation
- Characteristic granular pattern of staining of GBM and or mesangium for immunoglobulin and/or complement
- Disorder usually does not respond to plasmapheresis
§ 3. Pauci-immune type crescentic GN
- Lack of anti-GBM antibodies
- Antineutrophil cytoplasmic antibodies (ANCA) found in serum
Q’j$,&’D$”(“’q+*”($”(’*”’%*=*-(+’-1’-/(’8*+,(&
.
Clinical presentation
1’t,”(-’=#D/’%*8(’,(?/0*-*D’”&,+01=(q’1%*M#0*$’$,+’$c1-(=*$’=10(’?01=*,(,- o Proteinuria sometimes approaching nephrotic range
1’R1=(’$CC(D-(+’q’$,#0*$’$,+’0(u#*0(’%1,M9-(0=’+*$%&”*”’10’-0$,”?%$,-$-*1,
1’d0(+*D-*1,q’*C’D0(“D(,-’$0(’?0(“(,-’*,’x3B5’q=10(’C$)1#0$>%(
Diagnosis o Serum analysis
y’Y,-*9M%1=(0#%$0’>$”(=(,-’=(=>0$,(’$,-*>1+*(“’qf&?(’% y’Y,-’”-0(?-1%&”*,’t’$,-*>1+*(“6’$,-*9g@Y’$,-*>1+*(“6’D0&1M%1>#%*,”q’f&?(’L y’Y@FY’-*-0(’q-&?(p o Progressive renal failure over weeks or months 1’R(0#=’D0($-*,(’q$%=1”-’$%.$&”’(%()$-(+
1’!0*,$%&”*”q’/(=$-#0*$6’ZXF’D$”-“’?0(“(,- o Complement measurement o Early renal biopsy y’[1D$%’?01%*C(0$-*1,’1C’M%1=(0#%$0’(?*-/(%*$%’D(%%”’*,-(0”?(0″(+’.*-/’,(#-01?/*%”’q’ D0(“D(,-*D cellular mass
y’h%1=(0#%$0’-#C-’q’/&?1D(%%#%$0z’,(D01″*”’=$&’1DD#0
81. Chronic glomerulonephritis – etiology, pathogenesis, morphology, forms, clinical presentation, diagnosis.
Glomerulonephritis, is a renal involvement of both kidneys on an immune basis characterized by inflammation of the glomeruli and small blood vessels
Presentation may be with:
1.isolated hematuria and/or proteinuria)
- or with a massive proteinuria (nephrotic syndrome),
- or with hypertension and hematuria and azotemia (nephritic syndrome), 4. or as acute renal failure,
5. or chronic renal failure.
Chronic glomerulonephritis: One of a group of kidney diseases characterized by longterm inflammation and scarring of the glomeruli (microscopic structures in the kidney that filter blood and produce urine). This form of kidney disease usually develops slowly (over years) and may not produce symptoms at the outset. When symptoms and signs do appear, they typically include blood in the urine (hematuria), swelling (edema), high blood pressure, foamy urine (due to protein content), and frequent nighttime urination.
Etiology
A number of different medical conditions can cause chronic glomerulonephritis. Hereditary conditions may be responsible, or immune diseases may be the cause. In many cases, the exact cause is not apparent. Chronic glomerulonephritis may progress to kidney failure in some cases. Hypertension and diabetes are two conditions that typically result in scarring of the glomeruli and decline in kidney function. Pathogenesis represents progressive and irreversible destruction of kidney structures
- Caused by permanent loss of nephrons, including diabetes, hypertension, glomerulonephritis,and polycystic kidney disease – Amazing compensatory ability of the kidneys
- Typically, the signs and symptoms of renal failure occur when the disease is far advanced
- The remaining nephrons undergo structural and functional hypertrophy, each increasing its function as a means of compensating for those that have been lost – When the few remaining nephrons are destroyed that the manifestations of renal failure become evident
- Progressive decrease of glomerular filtration, tubular reabsorptive capacity, and endocrine functions of the kidneys and reduction in the GFR, reflecting a corresponding reduction in the number of functional nephrons occurs
Forms
- Non Proliferative
- Minimal change GN (also known as Minimal Change Disease)
- Focal Segmental Glomerulosclerosis (FSGS)
- Membranous glomerulonephritis
- Proliferative
- IgA nephropathy (Berger’s disease)
- Membranoproliferative/mesangiocapillary GN
2.3Rapidly progressive glomerulonephritis Clinical presentation glomerulonephritis signs and symptoms include:
-
- Pink or cola-colored urine from red blood cells in your urine (hematuria)
- Foamy urine due to excess protein (proteinuria)
- High blood pressure (hypertension)
- Fluid retention (edema) with swelling evident in your face, hands, feet and abdomen
Diagnosis
Glomerulonephritis often comes to light when a routine urinalysis is abnormal. Tests to assess your kidney function and make a diagnosis of glomerulonephritis include:
-
- Urine test. A urinalysis might show red blood cells and red cell casts in your urine, an indicator of possible damage to the glomeruli. Urinalysis results might also show white blood cells, a common indicator of infection or inflammation, and increased protein, which can indicate nephron damage. Other indicators, such as increased blood levels of creatinine or urea, are red flags.
- Blood tests. These can provide information about kidney damage and impairment of the glomeruli by measuring levels of waste products, such as creatinine and blood urea nitrogen.
- Imaging tests. If your doctor detects evidence of damage, he or she may recommend diagnostic studies that allow visualization of your kidneys, such as a kidney X-ray, an ultrasound exam or a CT scan.
- Kidney biopsy. This procedure involves using a special needle to extract small pieces of kidney tissue for microscopic examination to help determine the cause of the inflammation. A kidney biopsy is almost always necessary to confirm a diagnosis of glomerulonephritis.
82. Acute and chronic pyelonephritis – etiology, pathogenesis, morphology diagnosis.
Acute pyelonephritis is a sudden and severe kidney infection. It causes the kidneys to swell and may permanently damage them. Pyelonephritis can be life-threatening.
When repeated or persistent attacks occur, the condition is called chronic pyelonephritis. The chronic form is rare, but it happens more often in children or people with urinary obstructions.
ETIOLOGY
| ● | Usually caused by an ascending bacterial infection of the bladder (cystitis) |
| ● | Less commonly due to hematogenous spread of infection to the kidney (e.g., infectious endocarditis) |
| ● | Pathogens |
○ Gram-negative bacteria
■ Escherichia coli’Eb’74‘wB5’1C’D$”(“z’%($+*,M’D$#”(’1C’?&(%1,(?/0*-*”G
○ Gram-positive bacteria
■ Enterococcus faecalis
■ Staphylococcus saprophyticus [1]
○ Candida infection (especially in immunocompromised patients) is possiblE
PATHOGENESIS
The infection usually starts in the lower urinary tract as a urinary tract infection (UTI). Bacteria enter the body through the urethra and begin to multiply and spread up to the bladder. From there, the bacteria travel through the ureters to the kidneys.
Bacteria such as E. coli often cause the infection. However, any serious infection in the bloodstream can also spread to the kidneys and cause acute pyelonephritis. Chronic forms of the condition are more common in people with urinary obstructions. These can be caused by UTIs, vesicoureteral reflux, or anatomical anomalies. Chronic pyelonephritis is more common in children than in adults.
CLINICAL PRESENTATION
Symptoms usually appear within two days of infection. Common symptoms include:
- a fever greater than 102°F (38.9°C)
- painful or burning urination
- cloudy urine
- pus or blood in the urine
- urgent or frequent urination
- fishy-smelling urine
| ● | Chills |
| ● | Flank pain |
| ● | Costovertebral angle tenderness: pain upon percussion of the flank (usually unilateral, may be bilateral) |
| ● | Dysuria as well as other symptoms of cystitis (e.g., frequency, urgency) |
| ● | Weakness, nausea, vomiting (diarrhea may also be present) |
| ● | Possible abdominal or pelvic pain |
MORPHOLOGY
Acute pyelonephritis
Most commonly affects the cortex (spares glomeruli and vessels)
Purulent inflammation of the interstitium with destruction of the parenchyma, the renal tubules, and, in some cases, the renal pelvis
Neutrophilic infiltration of the renal tubules and the interstitium
Sparing of the glomeruli and intrarenal vessels
Chronic inflammatory changes with rough, asymmetric scarring and fibrosis of the corticomedullary junction
Blunted calyces from recurrent urinary reflux
Histology: eosinophilic casts in the tubules that resemble thyroid tissue with colloid (thyroidization of the kidney)
DIAGNOSIS
- Urine tests
- Imaging tests
- Radioactive imaging
Additional blood tests
| ● | CBC: leukocytosis |
| ● | Inflammatory markerso’V’CRP, ESR |
| ● | BMP: may be normal or show elevated BUN and creatinine |
83. Nephrolithiasis – etiology, pathogenesis, clinical presentation, diagnosis.
Nephrolithiasis encompasses the formation of all types of urinary calculi in the kidney, which may deposit along the entire urogenital tract from the renal pelvis to the urethra.
Epidemiology
- Sex: ♂ > ♀, Peak incidence: 30–60 years
- Risk factors
○ Low fluid intake, dehydration
○ Personal or family history
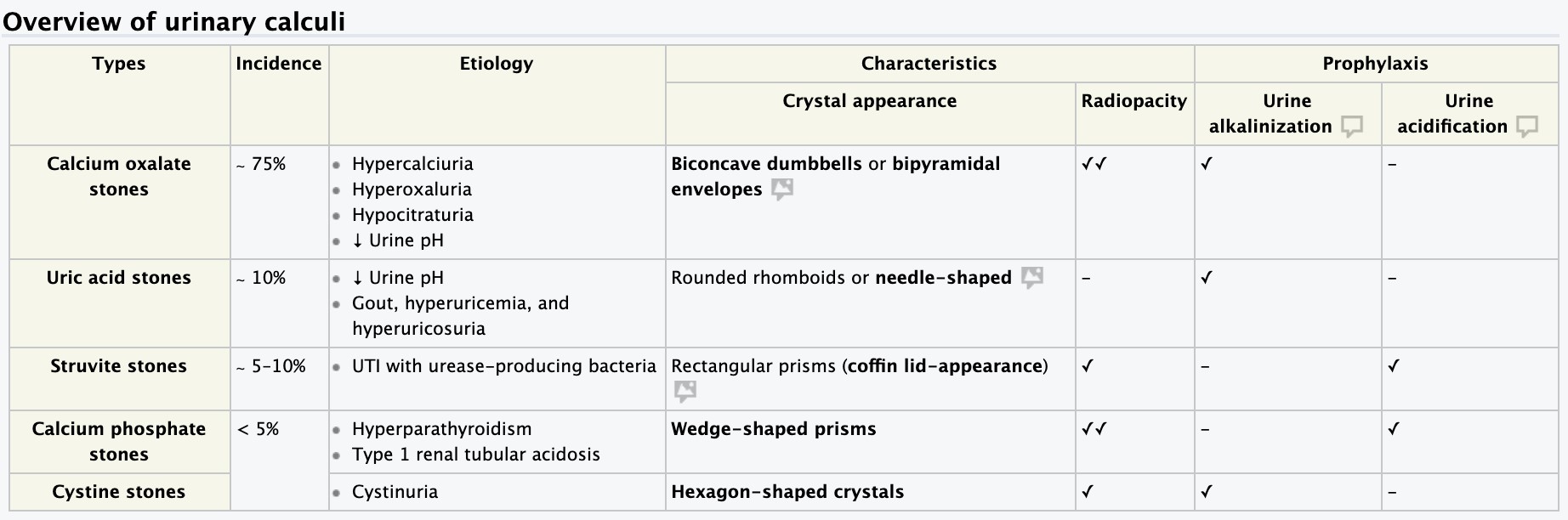
Clinical features
Stones usually form in the collecting ducts of the kidneys but may be deposited along the entire urogenital tract from the renal pelvis to the urethra. Their localization and size determine the specific symptoms. Small kidney stones may also be asymptomatic and detected incidentally.
- Severe unilateral and colicky flank pain (renal colic)
○ Radiates anteriorly to the lower abdomen, groin, labia, testicles, or perineum
○ Paroxysmal or progressively worsening
○ The area around the kidneys may be tender on percussion (costovertebral angle tenderness)
- Hematuria
- Nausea, vomiting, and reduced bowel sounds
- Dysuria, frequency, and urgency
- Passage of gravel or a stone
Diagnostics
Initial : imaging studies to locate the stone and laboratory tests to determine kidney function and assess for UTI.
- Laboratory tests
◆ V’WBC: suggests concomitant UTI
◆ V’R(0#=’#0($’,*-01M(,’$,+’creatinine: suggests acute kidney injury
◆ Urine dipstick and urinalysis
-
- Gross or microscopic hematuria
- Pyuria, positive leukocyte esterase, positive nitrites, or bacteriuria (suggests UTI)
- Urine pH
○ > 7 suggests urea-splitting organisms and struvite stones
○ < 5 indicates uric acid stones
● Urine microscopy: may detect crystals
○ Dumbbell-shaped or octahedron-shaped crystals indicate calcium oxalate stones
○ Rhomboid/needle-shaped crystals indicate uric acid stones
○ Rectangular prisms (coffin lid-appearance) indicate struvite stones
◆ Urine culture: obtain in patients with clinical or laboratory signs of UTI
◆ Straining of urine: enables chemical analysis of stone composition and specific guidance on preventive treatment (see prevention section below)
◆ Metabolic evaluation: indicated in recurrent stones formers and high-risk first-time stone formers
-
- Serum calcium, phosphorus, uric acid, bicarbonate, PTH, albumin, and alkaline phosphate: to detect metabolic abnormalities
- Twenty-four-hour urine profile: to analyze urine compounds
- Imaging
◆ Non Enhanced abdominopelvic CT scan: (gold standard) Demonstrates calculus size, site, density , and degree of obstruction
- Hydronephrosis: dilatation of the urinary tract proximal to the site of obstruction
◆ Ultrasound: method of choice for patients in whom radiation exposure should be minimized (e.g., pregnant patients, children, recurrent stone formers) or if a gynecological or abdominal differential diagnosis is likely
◆ Kidney, ureter, and bladder (KUB) X-ray
- X-ray positive (radiopaque): calcium-containing stones
- Weakly x-ray positive: struvite stones, cystine stones
- X-ray negative (radiolucent): uric acid stones
◆ Intravenous pyelogram (IVP)
Treatment
Approach considerations
- Determine if it is a complicated case, including: high-grade or infected hydronephrosis, urosepsis, acute kidney injury, intractable pain, or vomiting
- S(=1+&,$=*D$%%&’”-$>%(’?$-*(,-“’.*-/’#,D1=?%*D$-(+’”-1,(“’2’KB’==’q’$’-0*$%’1C’
1>”(0)$-*1,’.*-/’”&=?-1=$-*D’-0($-=(,-’-1’(,$>%(’”?1,-$,(1#”’?$””$M(
- Urological intervention required for:
○ Patients with stones > 10 mm
○ Complicated stones
○ Patients who decline conservative treatment
○ Failure to pass the stone spontaneously after 4–6 weeks
- For most patients with kidney’10’#0(-(0$%’”-1,(“’2’LB’==6’C*0”-9%*,(’*,-(0)(,-*1,$%’-0($-=(,-“’
*,D%#+(’>1-/’ureterorenoscopy and shock wave lithotripsy.
- For patient with kidney stones > 20 mm, percutaneous nephrolithotomy is preferred.
Medical therapy
- !,D1=?%*D$-(+’”-1,(“’2’KB’==o’1CC(0’1>”(0)$-*1,’.*-/’”&=?-1=$-*D’-0($-=(,-’$,+6’
(“?(D*$%%&’*,’D$”(’1C’distal ureteral stones > 5 mm, medical expulsive therapy
- Hydration
○ Analgesia (NSAIDs, IV morphine)
○ Medical expulsive therapy: alpha blockers (e.g., tamsulosin) or calcium-channel blockers (e.g., nifedipine)
○ Antibiotics: indicated in case of concomitant UTI
- Uric acid stones: dissolve with urine alkalinization
Urological intervention
- Indications
- Stones > 10 mm
○ Complicated stones, i.e., concomitant high-grade obstruction, urosepsis, impending acute kidney injury, intractable pain vomiting
○ After failed medical therapy, relapse, recurrent infection, or if preferred by patient
- Procedures
- Ureteral stenting or percutaneous nephrostomy : Surgical decompression in case of severely obstructed or infected pyelon; in those cases, definite stone treatment should be delayed until the infection has resolved.
○ Extracorporeal shock wave lithotripsy (SWL)
■ [*0″-9%*,(’-0($-=(,-’1?-*1,’C10’0(,$%’”-1,(“’2’LB’==’’$,+’#0(-(0$%’”-1,(“
■ Lowest complication rate but often repeated SWL is necessary for patients with residual stone burden
■ Stones have to be clearly visible on x-ray and/or ultrasound
■ Contraindicated in case of untreated UTI, during pregnancy, and in patients with bleeding diathesis; not preferred in morbidly obese patients ○ Ureterorenoscopy (URS) :
■ [*0″-9%*,(’-0($-=(,-’1?-*1,’C10’0(,$%’”-1,(“’2’LB’==’$,+’#0(-(0$%’”-1,(“
■ Greatest stone-free rate
○ Percutaneous nephrolithotomy : first-line treatment for renal stones > 20 mm
○ Laparoscopic or open stone removal (pyelolithotomy or ureterolithotomy): only considered in rare cases where other interventional methods have previously failed or
are likely to do so (e.g., because of complex staghorn stones)
Complications
- Recurrent urinary tract infections’q’0*”8’1C’pyelonephritis, urosepsis, and perinephric abscess
- Urinary obstruction’q’inflammation of the kidney (hydronephrosis’G’q’?(0=$,(,-’ M%1=(0#%$0’+$=$M(’*C’%(C-’#,-0($-(+
- Acute kidney injury
Prevention
- R#CC*D*(,-’C%#*+’*,-$8(’ET’L:4’ON+$&G’
- For calcium stones:
○ Reduced consumption of salt and animal protein
○ Reduced consumption of oxalate-rich foods and supplemental vitamin C: for oxalate stones
○ Thiazide diuretics for recurrent calcium-containing stones with idiopathic hypercalciuria (i.e., no hypercalcemia)
- For uric acid stones or high urinary uric acid levels in those with calcium stones: allopurinol
- Depending on urinary pH and stone composition: urine alkalinization or acidification
84. Kidney tumors – clinical presentation, diagnosis.
Kidney cancer — also called renal cancer — is a disease in which kidney cells become malignant (cancerous) and grow out of control, forming a Tumor. Almost all kidney cancers first appear in the lining of tiny tubes (tubules) in the kidney. This type of kidney cancer is called renal cell carcinoma.
Types
1. Renal cell carcinoma
• derived from renal tubular epithelium
Q’F%($0’D(%%’D$0D*,1=$”’qD(%%”’.*-/’D%($0’D&-1?%$”=’q’&(%%1.’-1’10$,M(’-1’./*-(’q cystic softening or hemorrhage, mainly arise from the proximal tubules Q’d$?*%%$0&’0(,$%’D(%%’D$0D*,1=$”’q’C*>01)$”D#%$0’D10(“’6’-(,+’-1’>(’>*%$-(0$%’$,+ multifocal
2. Wilms Tumor embryonic, nephroblastoma
- Common primary neoplasms of young children
- Presenting signs large asymptomatic abdominal mass and hypertension, but can have ● abdominal pain and vomiting
Clinical presentation
- Silent disorder during early stages, symptoms appear in late stages
1’F%$””*D’-0*$+’q?$*,%(“”’E’=$D01’10’=*D01G’/(=$-#0*$6’+#%%’C%$,8’?$*,6’?$%?$>%(’=$””’*, o abdomen
- Loss of appetite o Weight loss o Tiredness o Fever o Anaemia
1’f#=10’D$,’?01+#D(’1-/(0’/10=1,(9%*8(’”#>”-$,D(“’%($+*,M’-1’S&?(08$%(=*$6’/&?(0-(,”*1,6’ F#”/*,M’”&,+01=(’10’C(=$%(’10’=$”D#%*,*c$-*1,q’?$0$,(1?%$”-*D’”&,+01=(
Diagnosis o blood and urine tests
- Imaging tests–. Ultrasound, CT, MRI o biopsy
1’D/(“-’r90$&’q=(-$”-$”*” o renal arteriography
1’>1,(’”D$,’q=(-$”-$”*”’10’D/(D8’$%8$%*,(’?/1″?/$-$”(’%()(%”
- positron emission tomography imaging (PET)
85. Diseases of the esophagus (functional diseases, esophagitis, carcinoma) – etiology, pathogenesis, clinical presentation, diagnosis.
Heartburn (pyrosis), the most common esophageal symptom, is characterized by a discomfort or burning sensation behind the sternum that arises from the epigastrium and may radiate toward the neck. Heartburn is an intermittent symptom, most commonly experienced after eating, during exercise, and while lying recumbent. The discomfort is relieved with drinking water or antacid but can occur frequently interfering with normal activities including sleep. The association between heartburn and gastroesophageal reflux disease (GERD) is so strong that empirical therapy for GERD has become accepted management. However, the term “heartburn” is often misused and/or referred to with other terms such as “indigestion” or “repeating,” making it important to clarify the intended meaning.
Regurgitation is the effortless return of food or fluid into the pharynx without nausea or retching. Patients report a sour or burning fluid in the throat or mouth that may also contain undigested food particles. Bending, belching, or maneuvers that increase intra abdominal pressure can provoke regurgitation.
Chest pain is a common esophageal symptom with characteristics similar to cardiac pain, sometimes making this distinction difficult. Esophageal pain is usually experienced as a pressure type sensation in the mid chest, radiating to the mid back, arms, or jaws. The similarity to cardiac pain is likely because the two organs share a nerve plexus and the nerve endings in the esophageal wall have poor discriminative ability among stimuli. Esophageal distention or even chemo stimulation (e.g., with acid) will often be perceived as chest pain. Gastroesophageal reflux is the most common cause of esophageal chest pain.
Esophageal dysphagia is often described as a feeling of food “sticking” or even lodging in the chest. Important distinctions are between uniquely solid food dysphagia as opposed to liquid and solid, episodic versus constant dysphagia, and progressive versus static dysphagia. If the dysphagia is for liquids as well as solid food, it suggests a motility disorder such as achalasia. Conversely, uniquely solid food dysphagia is suggestive of a stricture, ring, or tumor. Of note, a patient’s localization of food hang-up in the esophagus is notoriously imprecise. Approximately 30% of distal esophageal obstructions are perceived as cervical dysphagia. In such instances, the absence of concomitant symptoms generally associated with oropharyngeal dysphagia such as aspiration, nasopharyngeal regurgitation, cough, drooling, or obvious neuromuscular compromise should suggest an esophageal etiology.
Odynophagia is pain either caused by or exacerbated by swallowing. Although typically considered distinct from dysphagia, odynophagia may manifest concurrently with dysphagia. Odynophagia is more common with pill or infectious esophagitis than with reflux esophagitis and should prompt a search for these entities. When odynophagia does occur in GERD, it is likely related to an esophageal ulcer or extensive erosions.
Globus sensation, also known as globus pharyngeus, is the perception of a lump or fullness in the throat that is felt irrespective of swallowing. Although such patients are frequently referred for an evaluation of dysphagia, globus sensation is often relieved by the act of swallowing. As implied by its alternative name, “globus hystericus,” globus sensation often occurs in the setting of anxiety or obsessive-compulsive disorders. Clinical experience teaches that it is often attributable to GERD.
Water brash is excessive salivation resulting from a vagal reflex triggered by acidification of the esophageal mucosa. This is not a common symptom. Afflicted individuals will describe the unpleasant sensation of the mouth rapidly filling with salty thin fluid, often in the setting of concomitant heartburn.
Etiology
Genetic, CMV, herpetic esophagitis, candida esophagitis
Pathophysiology
Esophagitis occurs when refluxed gastric acid and pepsin cause necrosis of the esophageal mucosa causing erosions and ulcers. Note that some degree of gastroesophageal reflux is normal, physiologically intertwined with the mechanism of belching (transient LES relaxation), but esophagitis results from excessive reflux, often accompanied by impaired clearance of the refluxed gastric juice. Restricting reflux to that which is physiologically intended depends on the anatomic and physiologic integrity of the esophagogastric junction, a complex sphincter comprising both the LES and the surrounding crural diaphragm. Three dominant mechanisms of esophagogastric junction incompetence are recognized: (1) transient LES relaxations (a vagovagal reflex in which LES relaxation is elicited by gastric distention), (2) LES hypotension, or (3) anatomic distortion of the esophagogastric junction inclusive of hiatus hernia. Of note, the third factor, esophagogastric junction anatomic disruption, is both significant unto itself and also because it interacts with the first two mechanisms. Transient LES relaxations account for about 90% of reflux in normal subjects or GERD patients without hiatus hernia, but patients with hiatus hernia have a more heterogeneous mechanistic profile. Factors tending to exacerbate reflux regardless of mechanism are abdominal obesity, pregnancy, gastric hypersecretory states, delayed gastric emptying, disruption of esophageal peristalsis, and gluttony.
After acid reflux, peristalsis returns the refluxed fluid to the stomach and acid clearance is completed by titration of the residual acid by bicarbonate contained in swallowed saliva. Consequently, two causes of prolonged acid clearance are impaired peristalsis and reduced salivation. Impaired peristaltic emptying can be attributable to disrupted peristalsis or superimposed reflux associated with a hiatal hernia. With superimposed reflux, fluid retained within a sliding hiatal hernia refluxes back into the esophagus during swallow-related LES relaxation, a phenomenon that does not normally occur.
Clinical symptoms
Heartburn and regurgitation are the typical symptoms of GERD. Somewhat less common are dysphagia and chest pain. In each case, multiple potential mechanisms for symptom genesis operate that extend beyond the basic concepts of mucosal erosion and activation of afferent sensory nerves. Specifically, hypersensitivity and functional pain are increasingly recognized as cofactors. Nonetheless, the dominant clinical strategy is empirical treatment with acid inhibitors, reserving further evaluation for those who fail to respond. Important exceptions to this are patients with chest pain or persistent dysphagia, each of which may be indicative of more morbid conditions. With chest pain, cardiac disease must be carefully considered. In the case of persistent dysphagia, chronic reflux can lead to the development of a peptic stricture or adenocarcinoma, each of which benefits from early detection and/or specific therapy.
Barrett’s metaplasia leads to adenocarcinoma.
Diagnosis
Barium X-ray
For this test, you drink a solution containing a compound called barium or take a pill coated with barium. Barium coats the lining of the esophagus and stomach and makes the organs visible. These images can help identify narrowing of the esophagus, other structural changes, a hiatal hernia, tumors or other abnormalities that could be causing symptoms.
Endoscopy
Doctors guide a long, thin tube equipped with a tiny camera (endoscope) down your throat and into the esophagus. Using this instrument, your doctor can look for any unusual appearance of the esophagus and remove small tissue samples for testing. The esophagus may look different depending on the cause of the inflammation, such as drug-induced or reflux esophagitis. You’ll be lightly sedated during this test.
Laboratory tests
Small tissue samples removed (biopsy) during an endoscopic exam are sent to the lab for testing. Depending on the suspected cause of the disorder, tests may be used to:
- Diagnose a bacterial, viral or fungal infection
- Determine the concentration of allergy-related white blood cells (eosinophils)
- Identify abnormal cells that would indicate esophageal cancer or precancerous changes
86. Acute gastritis – etiology, pathogenesis, pathomorphology, clinical diagnosis.
ETIOLOGY
Acute gastritis occurs when the lining of your stomach is damaged or weak. This allows digestive acids to irritate the stomach. There are many things that can damage your stomach lining. The causes of acute gastritis include:
- medications such as nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroids
- bacterial infections such as H. pylori
- excessive alcohol consumption
NSAIDs and corticosteroids (steroid hormone medications) are the most common causes of acute gastritis.
H. pylori is a type of bacteria that can infect the stomach. It’s often the cause of peptic ulcers. While it’s unclear how H. pylori spreads, it can result in stomach inflammation, loss of appetite, nausea, bloating, and abdominal pain.
Other causes that are less common include:
- viral infections
- extreme stress
- autoimmune disorders, which may cause the immune system to attack the stomach lining
- digestive diseases and disorders such as Crohn’s disease
- bile reflux
- cocaine use
- ingesting corrosive substances such as poison
- surgery
- kidney failure
- systemic stress
- being on a breathing machine or respirator
PATHOGENESIS
Acute Gastritis does not refer to a unique pathophysiological entity but is rather a histological description of acute inflammation occurring in the gastric mucosa. Bouts of acute gastritis are typically transient; however, the pathogenesis is poorly understood. Several general mechanisms may contribute to the development of acute gastritis including increased stomach acid production and reduced bicarbonate production along with reduced blood flow or direct injury to the gastric mucosa.
PATHOMORPHOLOGY
Depending on the etiology, histological signs of acute gastritis may be focal or diffuse and are characterized by a neutrophilic infiltration of the gastric mucosa. Frequently, the gastric epithelium, and in more severe cases the gastric mucosa, is eroded. Although technically this would be considered an ulceration, the term acute gastric ulceration is reserved for a distinct pathological entity which is defined as ulceration past the gastric mucosa and into the gastric submucosa.
CLINICAL
Common symptoms include:
- loss of appetite
- indigestion
- black stools
- nausea
- vomiting
- bloody vomit that looks like used coffee grounds
- pain in the upper part of the abdomen
- a full feeling in the upper abdomen after eating
DIAGNOSIS
- a complete blood count (CBC), which is used to check your overall health
- a blood, breath, or saliva test, which is used to check for H. pylori
- a fecal test, which is used to check for blood in your stool
- an esophagogastroduodenoscopy, or endoscopy, which is used to look at the lining of your stomach with a small camera
- a gastric tissue biopsy, which involves removing a small piece of stomach tissue for analysis
- an X-ray, which is used to look for structural problems in your digestive system
87. Chronic gastritis – etiology, pathogenesis, pathomorphology, forms, clinical presentation, diagnosis.
Chronic gastritis is a long-term condition in which the mucus lined layer of the stomach, also known as the gastric mucosa, is inflamed or irritated over a longer period of time.
Pathogenesis:
- Identified histologically by an inflammatory cell infiltrate dominated by lymphocytes and plasma cells with scant neutrophils.
- In its early stage, the changes are limited to the lamina propria (superficial gastritis).
- When the disease progresses to destroy glands, it becomes atrophic gastritis. The final stage is gastric atrophy, in which the mucosa is thin and the infiltrate sparse. Chronic gastritis can be classified based on predominant sites of involvement.
Type A Gastritis (Autoimmune)
This is the body-predominant and less common form. Generally asymptomatic, common in elderly; autoimmune mechanism may be associated with achlorhydria, pernicious anemia, and increased risk of gastric cancer (value of screening endoscopy uncertain). Antibodies to parietal cells present in >90%.
- The body’s autoimmune response causes an inflammation of the protective mucus covered lining of the stomach, which eventually affects and degrades the mucusproducing cells.
- This leads to fewer mucus-producing cells being available and, consequently, less protection for the stomach. This is accompanied by a loss of parietal cells in the stomach, which regulate stomach acid. Parietal cells also affect absorption of vitamin B12 and iron by the stomach.
- So damage or loss of these cells may cause the body to have less vitamin B12 and iron available for its various processes and therefore lead to anemia and other deficiency symptoms
Type B Gastritis
This is an antral-predominant disease and caused by H. pylori. Often asymptomatic but may be associated with dyspepsia. Atrophic gastritis, gastric atrophy, gastric lymphoid follicles, and gastric B cell lymphomas may occur. Infection early in life or in setting of malnutrition or low gastric acid output is associated with gastritis of entire stomach (including body) and increased risk of gastric cancer. Eradication of H. pylori is not routinely recommended unless PUD or gastric mucosa-associated lymphoid tissue (MALT) lymphoma is present.
Also be caused by several chemical substances. These causes include:
- Repeated, high dose and/or prolonged use of certain pain-relievers such as aspirin, which may also be prescribed for non-pain treatment in lower doses, e.g., after a heart attack, or NSAID drugs such as ibuprofen or naproxen- Excessive consumption of alcohol.
- Bile, a liquid the liver produces to aid digestion, entering the stomach. This is known as bile reflux
- Other causes: stress, alcohol, cocaine use
Symptoms
- indigestion
- a burning or gnawing feeling in the stomach
- the sensation of being full after eating a small amount
- nausea and vomiting, belching, bloating
- unintentional weight loss, loss of appetite
- upper abdominal pain or discomfort
- bleeding, usually only in erosive gastritis Diagnosis:
- Medical history – inc, use of medications such as aspirin, NSAID pain-relievers and antacids, as well as alcohol consumption and travel to countries where infection with H. pylori is common.
- The doctor will also conduct a physical examination of the abdomen/belly.
- Depending on these factors, a number of tests may be used for helping with diagnosis or evaluating potential causes:
| Testing for H. pylori | : |
| Blood tests for anemia | |
| Blood tests to find antibodies |
● These tests may include a blood, stool or breath tests
●
| Liver and kidney function blood tests |
| Stool tests for the presence of blood |
●:that mistakenly provoke an immune response against cells in a person’s own stomach ● ●
- Other tests may include:
- EGD (esophagogastroduodenoscopy), also called gastroscopy or upper endoscopy: An EGD is a visual inspection of the stomach lining, performed by passing an endoscope – a long, thin, flexible tube with a lighted camera – down the throat and into the esophagus, stomach and upper small intestine.
– The doctor can examine the stomach lining for signs of inflammation and take a small tissue sample (biopsy) to test for H. pylori.35 An EGD is the best diagnostic tool for autoimmune chronic gastritis.6
- Upper gastrointestinal (GI) series: Also called a barium swallow, this test creates a series of X-rays of the GI tract. Swallowing a liquid containing barium (a metal compound) coats the inside of the stomach, esophagus and small intestine to make the organs, as well as any potential ulcer presence, polyps or other abnormality, more visible by X-ray. Treatment for chronic gastritis Depends on the underlying cause.
- If the condition is caused by prolonged and excessive use of NSAIDs or alcohol, the person will need to stop taking those substances.
- Assist with replacement painkillers or with any withdrawal effects and also redirect to other needed support, e.g., support groups for quitting alcohol.
Currently, there is no treatment available that will cure autoimmune chronic gastritis. However, the vitamin B12 and iron deficiencies that it often causes can be treated with supplements, in the form of tablets, shots or intravenous infusions.
88. Peptic ulcer – etiology, pathogenesis, clinical presentation, forms, complications, diagnosis
Peptic ulcer disease (PUD) refers to the presence of one or more ulcerative lesions in the stomach or lining of the duodenum. Possible etiologies include infection with the bacterium Helicobacter pylori (most common), prolonged use of nonsteroidal anti-inflammatory medicines (possibly in combination with glucocorticoids), conditions associated with an overproduction of stomach acid (hypersecretory states), and stress. Epigastric pain is a typical symptom of PUD, however, some patients may remain asymptomatic.
CLASSIFICATION
Gastric ulcer: an ulcerative lesion in the stomach lining; typically manifests along the lesser curvature and the gastric antrum
Duodenal ulcer: an ulcerative lesion located in the duodenum, typically in the first part (i.e., the duodenal bulb)
Erosive gastritis: acute mucosal inflammation of the stomach that does not extend beyond the muscularis mucosae
- A group of ulcerative disorders are exposed to acid-pepsin secretions Open sores on the inside lining
- Includes peptic ulcers and duodenal ulcers. Zollinger-Ellison syndrome in duodenum, stomach
+/ jejunum o Breach in mucosa that extends through the muscularis mucosa and submucosa/ deeper o Peptic ulcers are chronic, most often solitary lesions (< 4 cm) that occur in an portion of the GIT exposed to acid/ peptic juices
Etiology o H. pylori (70-90%)
- Chronic use of NSAIDs (e.g. aspirin, ibuprofen) o Risk factors: smoking, alcohol, severe physiologic stress
• Pathogenesis o Imbalance between protective mucosal defences aggressive factors o Defensive factors
- Prostaglandins
- Mucous
- Bicarbonates
- Mucosal blood flow o Aggressive factors
- Pepsin
- HCI
o NSAIDs
- Mucosal injury
- Inhibition of prostaglandin synthesis (PG increases bicarbonate + mucous production; ● vasodilator)
• Clinical presentation o 3/4 of people don’t have symptoms
- Most common Burning stomach pain (stomach acid and having an empty stomach makes it worse) – between meals and at night o Feeling of fullness, bloating/ belching o Fatty food intolerance o Heartburn and nausea- acid reflux
- Ulcer is located over a small area near the midline in the epigastrium near the xiphoid and may radiate below the costal margins, into the back rarely to the right shoulder
• Complications o Bleeding
- 15%-20% of patients, most frequent complication
- May be life-threatening, accounts for 25% of ulcer death
- First indication of an ulcer o Perforation of wall
o Obstruction from edema / scarring
- 2% of patients
- Most often due to pyloric channel ulcers and maybe also with duodenal ulcers
- Incapacitating, crampy abdominal pain
• Diagnosis o Laboratory test for H Pylori (same as for chronic gastritis) o Endoscopy, biopsy
- Upper Gl series: barium swallow, series of X-rays of your upper digestive system creates images of upper GIT
- Treatment: antibiotics, meds to block acid production (proton pump inhibitors), acid blockers, antacids
89. Gastric cancer. Etiology, pathogenesis, morphology, clinical presentation, forms diagnosis.
Etiology
Infection by Helicobacter pylori is believed to be the cause of most stomach cancer while autoimmune atrophic gastritis, intestinal metaplasia and various genetic factors are associated with increased risk levels. Alcohol as cause of cancer along with tobacco smoking as cause of cancer
Pathogenesis
The pathogenesis of these conditions is less well understood, although both arise in association with pan- or corpus-predominant gastritis. The hormonal changes described above still occur, but the tissue responses in the gastric corpus mean that it produces less acid (hypochlorhydria) despite hypergastrinemia. Gastric ulcers commonly occur at the junction of antral and corpus-type mucosa, an area that is often particularly inflamed. Gastric cancer probably stems from progressive DNA damage and the survival of abnormal epithelial cell clones. The DNA damage is thought to be due principally to reactive oxygen and nitrogen species arising from inflammatory cells, perhaps in relation to other bacteria that survive in a hypochlorhydria stomach. Longitudinal analyses of gastric biopsy specimens taken years apart from the same patient show that the common intestinal type of gastric adenocarcinoma follows stepwise changes from simple gastritis to gastric atrophy, metaplasia, and dysplasia. A second, diffuse type of gastric adenocarcinoma found more commonly in younger adults may arise directly from chronic gastritis without atrophic changes.
Clinical presentation asymptomatic or causes only nonspecific symptoms Stage 1 (Early):
Indigestion or a burning sensation (heartburn)
Loss of appetite, especially for meat
Abdominal discomfort or irritation
Stage 2 (Middle)
Weakness and fatigue
Bloating of the stomach, usually after meals
Stage 3 (Late)
Abdominal pain in the upper abdomen
Nausea and occasional vomiting
Diarrhea or constipation
Weight loss
Bleeding (vomiting blood or having blood in the stool) which will appear as black. This can lead to anemia.
Dysphagia; this feature suggests a tumor in the cardia or extension of the gastric tumor into the esophagus.
Diagnosis
Gastroscopic exam is the diagnostic method of choice. This involves insertion of a fiber optic camera into the stomach to visualize it.
Upper GI series (may be called barium roentgenogram)
Computed tomography or CT scanning of the abdomen
CT scan, a PET scan, an endoscopic ultrasound exam, or other tests to check these areas. Blood tests for tumor markers, such as carcinoembryonic antigen (CEA) Regional and distant lymph nodes Organ involvement-liver, bones, CNS
TNM system
Staging
Stage 0. Limited to the inner lining of the stomach. Treatable by endoscopic mucosal resection when found very early (in routine screenings); otherwise by gastrectomy and lymphadenectomy without need for chemotherapy or radiation.
Stage I. Penetration to the second or third layers of the stomach (Stage 1A) or to the second layer and nearby lymph nodes (Stage 1B). Stage 1A is treated by surgery, including removal of the omentum. Stage 1B may be treated with chemotherapy (5fluorouracil) and radiation therapy.
Stage II. Penetration to the second layer and more distant lymph nodes, or the third layer and only nearby lymph nodes, or all four layers but not the lymph nodes. Treated as for Stage I, sometimes with additional neoadjuvant chemotherapy.
Stage III . Penetration to the third layer and more distant lymph nodes, or penetration to the fourth layer and either nearby tissues or nearby or more distant lymph nodes. Treated as for Stage II; a cure is still possible in some cases.
Stage IV . Cancer has spread to nearby tissues and more distant lymph nodes, or has metastasized to other organs. A cure is very rarely possible at this stage. Some other techniques to prolong life or improve symptoms are used, including laser treatment, surgery, and/or stents to keep the digestive tract open, and chemotherapy by drugs such as 5- fluorouracil, cisplatin, epirubicin, etoposide, docetaxel, oxaliplatin, capecitabine, or irinotecan.
90. Acute and chronic colitis. Ulcerative colitis – etiology, pathogenesis, clinical presentation, diagnosis.
ETIOLOGY
Colitis refers to inflammation of the inner lining of the colon. There are numerous causes of colitis including infection, inflammatory bowel disease (Crohn’s disease and ulcerative colitis are two types of IBD), ischemic colitis, allergic reactions, and microscopic colitis.
The exact cause of ulcerative colitis remains unknown. Previously, diet and stress were suspected, but now doctors know that these factors may aggravate but don’t cause ulcerative colitis.One possible cause is an immune system malfunction. When your immune system tries to fight off an invading virus or bacterium, an abnormal immune response causes the immune system to attack the cells in the digestive tract, too. Heredity also seems to play a role in that ulcerative colitis is more common in people who have family members with the disease. However, most people with ulcerative colitis don’t have this family history.
PATHOGENESIS
CLINICAL PRESENTATION
- Diarrhea or loose stools
- Abdominal pain
- Urgent need to defecate
- Cramps
- Dehydration
- Bloody stools
Signs and symptoms of chronic ulcerative colitis can include:
- Persistent diarrhea or loose stools
- Bloody stools
- Abdominal pain
- Cramps
- Urgent need to defecate
- Dehydration
- Constipation ● Weight loss
- Brittle bones
- Malnutrition
- Fatigue
- Weakness
- Anemia
- Joint pain
- Skin and eye disorders
Doctors often classify ulcerative colitis according to its location. Types of ulcerative colitis include:
- Ulcerative proctitis. Inflammation is confined to the area closest to the anus (rectum), and rectal bleeding may be the only sign of the disease. This form of ulcerative colitis tends to be the mildest.
- Proctosigmoiditis. Inflammation involves the rectum and sigmoid colon (lower end of the colon). Signs and symptoms include bloody diarrhea, abdominal cramps and pain, and an inability to move the bowels in spite of the urge to do so (tenesmus).
- Left-sided colitis. Inflammation extends from the rectum up through the sigmoid and descending colon. Signs and symptoms include bloody diarrhea, abdominal cramping and pain on the left side, and unintended weight loss.
- Pancolitis. Pancolitis often affects the entire colon and causes bouts of bloody diarrhea that may be severe, abdominal cramps and pain, fatigue, and significant weight loss.
- Acute severe ulcerative colitis. This rare form of colitis affects the entire colon and causes severe pain, profuse diarrhea, bleeding, fever and inability to eat.
DIAGNOSIS
- BLOOD TESTS – A low red blood cell count can indicate anemia, from bleeding within the colon and rectum. Elevated white blood cells, which fight infection, indicate inflammation within the colon and rectum
- STOOL SAMPLE – A stool sample may be taken to rule out a parasitic infection that can cause colitis.
- CT SCAN
91. Colon cancer – etiology, pathogenesis, clinical presentation, diagnosis.
Epidemiology
- Incidence: Third most common cancer in women and men
- Age: continuous increase in incidence after the age of 50
- Mortality: third leading cause of cancer-related deaths in the US overall
Etiology
- Predisposing factors
- Colorectal adenomas
- Family history
- Hereditary syndromes
- Familial adenomatous polyposis: 100% risk by age 40
○ Hereditary nonpolyposis colorectal cancer (HNPCC): 80% progress to CRC.
- Conditions associated with an increased risk of colorectal cancer
- Inflammatory bowel disease (IBD): ulcerative colitis and Crohn’s disease
■ Chronic inflammation’q’hyperplasia’q’,1,9?1%&?1*+’+&”?%$”*$q’neoplasia
○ Endocarditis and bacteremia due to Streptococcus gallolyticus is associated with CRC.
- Diet and lifestyle
- Smoking
○ Alcohol consumption
○ Obesity
○ Processed meat; high-fat, low-fiber diets
- Older age
Clinical features
Often asymptomatic, particularly during the early stages of disease
- Nonspecific symptoms: constitutional symptoms (weight loss, fever, night sweats), fatigue, abdominal discomfort
- In general, right-sided tumors chronically bleed, and left sided tumors cause obstruction
| Symptoms according to location | Symptoms according to stage of disease | ||
| ○
○ ○ ○ | Rectosigmoid > ascending colon > descending colon
Right-sided carcinomas (10%): cecum and ascending colon ■ Iron deficiency anemia ■ Melena ■ Diarrhea Left-sided carcinomas (10%): transverse and descending colon ■ Changes in bowel habits (size, consistency, frequency) ■ Blood-streaked stools ■ Colicky abdominal pain due to obstruction Rectum (50%) and sigmoid (30%) ■ Hematochezia ■ W’R-11%’D$%*>(0’E?(,D*%9″/$?(+’”-11%G ■ Rectal pain ■ Tenesmus ■ Flatulence with involuntary stool loss | ○
○ | Advanced disease
■ Palpable abdominal mass ■ Intestinal obstruction or perforation Metastatic disease: 20% of patients already have distant metastasis on initial diagnosis. ■ Liver metastases : abdominal distention, hepatomegaly, ascites ■ Lung metastases : dyspnea, cough, hemoptysis, pleural effusion ■ Lymphatic spread to mesenteric, para-aortic, and pelvic lymph nodes |
Stages:
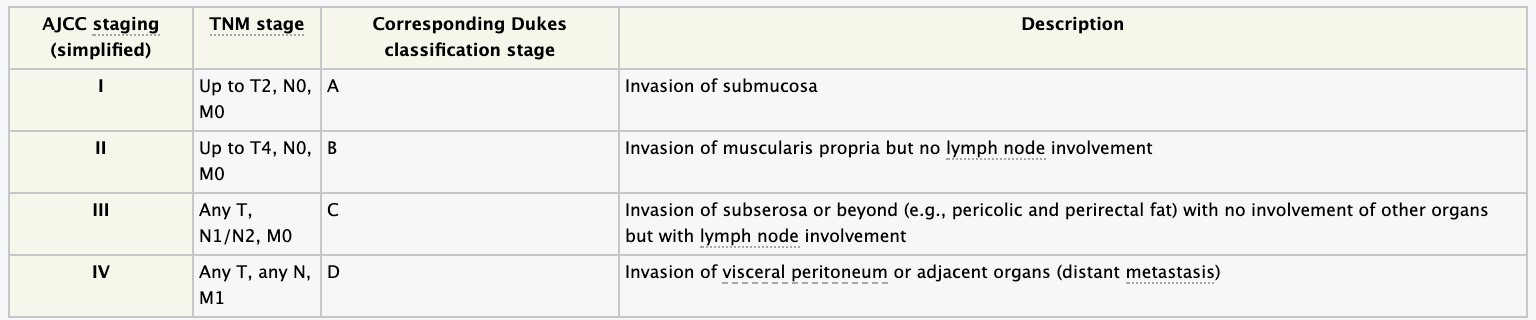
Diagnosis:
Initial work-up
- Digital rectal examination: Up to 10% of cancers are palpable!
- Complete colonoscopy: gold standard
Staging and further tests
- Determine the extent of local and distant disease
- Endorectal ultrasound: determine depth of tumor infiltration
○ CT of abdomen, pelvis, and chest, CXR
- Tumor marker: carcinoembryonic antigen (CEA) serum levels prior to initiating treatment
Treatment primarily depends on the location of the tumor and the TNM stage.
Colon cancer
- Curative approach: any primary tumor with or without regional spread; resectable metastases in the liver and/or lung
- Treatment involves surgical resection and adjuvant chemotherapy.
- Palliative approach: distant metastases beyond the liver and/or lung or if the patient is not a surgical candidate due to poor general health
- Treatment involves palliative chemotherapy.
Surgical management
- Colectomy: The extent of the resection depends on the location of the tumor.
- Regional lymph node dissection (for pathologic staging)
- Resection of resectable metastases in liver and/or lung
Systemic therapy
- Chemotherapy
- Biologicals: Anti-VEGF antibodies or EGFR antibody may be added to the chemotherapy regimen for metastatic disease.
- Radiation therapy: not a standard modality for treatment of colon cancer
92. Chronic hepatitis – etiology, pathogenesis, clinical presentation, diagnosis.
o Inflammation of the liver that lasts at least 6 months o Hepatitis may occur with limited or no symptoms but often leads to jaundice, anorexia malaise. o Hepatitis viruses cause most cases of hepatitis worldwide but it can also be due to toxins
(notably
alcohol, medications, some industrial organic solvents plants), other infections autoimmune diseases
Etiology
- Hepatitis C virus (60-70%): At least 75% of acute hepatitis C cases come chronic o Hepatitis B virus
- Fatty liver not due to alcohol use (non-alcoholic steatohepatitis) o Alcoholic hepatitis t o Autoimmune hepatitis o Drugs: methyldopa, nitrofurantoin, isoniazid, ketoconazole o Heredity: Wilson’s disease, alpha-1 antitrypsin deficiency
Pathogenesis
o Chronic persistent hepatitis: benign, self-limited; prolonged recovery. Asymptomatic except elevated transaminases
1’F/01,*D’$D-*)(’/(?$-*-*”o’D/01,*D’*,C%$==$-*1,’.*-/’/(?$-1D&-(’+(“-0#D-*1,’qD*00/1″*”’1C’%*)(0’ C$*%#0(
(portal tract areas). Histology is aggressive in appearance. o HBV, HCV+ HDV have the potential for progression to the carrier state, chronic hepatitis, cirrhosis and hepatocellular carcinoma
Clinical presentation
- Enlarged spleen/ liver, Redness of palms, Ascites
- Small spider like blood vessels visible in the skin (spider angiomas) o Deterioration of brain function (hepatic encephalopathy)
Diagnosis
o Blood tests liver biopsy
93. Liver cirrhosis – etiology, pathogenesis, classification, clinical picture, diagnosis.
Diffuse disorganization of normal hepatic structure by regenerative nodules that are surrounded by fibrotic tissue.The pathologic changes in cirrhosis generally involve the entire liver. Extensive fibrosis, even with regenerating nodules (ie, cirrhosis), is usually irreversible, although fibrosis in animals can resolve, depending on experimental design. In humans, cirrhotic damage is permanent; nodule regeneration is a vain attempt at repair. Fibrosis is not synonymous with cirrhosis, which also includes nodule formation and scarring sufficient to cause deteriorated liver function.
Etiology
In the Western world, cirrhosis is the third leading cause of death in patients aged 45 to 65 (after cardiovascular disease and cancer); most cases are secondary to chronic alcohol abuse. In many parts of Asia and Africa, cirrhosis resulting from chronic hepatitis B is a major cause of death. Hepatitis C and other forms of chronic hepatitis (from autoimmune chronic active hepatitis and certain drugs) result in cirrhosis. Metabolic causes include hemochromatosis, Wilson’s disease, 1-antitrypsin deficiency. Even diabetes mellitus has been associated with the development of cirrhosis. Prolonged biliary obstruction (secondary biliary cirrhosis), chronic venous outflow obstruction (eg, Budd- Chiari syndrome), and malnutrition can lead to cirrhosis. Cirrhosis of unknown etiology, termed cryptogenic, is diagnosed less frequently as more specific diagnoses (eg, chronic hepatitis C virus infection) become available. Primary biliary cirrhosis is a special autoimmune type of cirrhosis
Pathogenesis
Cirrhosis is the end stage of many forms of liver injury characterized initially by fibrosis. The progression of fibrosis to cirrhosis and the morphology of the cirrhosis depend on the extent of injury, the presence of continuing damage, and the response of the liver to damage. Cirrhosis is related not so much to the injurious agents as to the kind of injury and the liver’s response to it. The liver may be injured acutely and severely (as in submassive necrosis with hepatitis), moderately over months or years (as in biliary tract obstruction and chronic active hepatitis), or modestly but continuously (as in alcohol abuse). Cytokines and hepatic growth factors (eg, epidermal growth factor) are presumably responsible for the response to injury: fibrosis plus regenerating nodules. Disordered blood flow to the nodules and compression of hepatic venules by regenerating nodules, as well as new vessels, which connect the hepatic artery and portal vein to the hepatic venules, restoring the intrahepatic circulatory pathway, contribute to portal hypertension. Cirrhosis is not static; its features depend on the disease activity and stage. Morphologic classification of cirrhosis does little to reveal its cause. Classification
Clinical picture
Many patients with cirrhosis are asymptomatic for years. Others show generalized weakness, anorexia, malaise, and weight loss. With obstruction to bile flow, jaundice, pruritus, and xanthelasmas become prominent. Malnutrition is common, secondary to anorexia with poor food intake, fat malabsorption, and fat-soluble vitamin deficiency caused by the effects of reduced bile-salt excretion. A more dramatic presentation is massive upper GI bleeding from esophageal varices secondary to portal hypertension. The initial presentation may occasionally be that of hepatocellular failure with ascites or portal-systemic encephalopathy. A palpable, firm liver with a blunt edge is typical, but at times the liver is small and difficult to palpate. Regenerating nodules are only occasionally palpable.. Ascites may be present with portal hypertension, splenomegaly, and a collateral venous circulation. Other clinical signs may suggest chronic liver disease, particularly in alcoholics, but none is specific: muscle wasting, palmar erythema, Dupuytren’s contractures, vascular spiders (<10 may be normal), gynecomastia, parotid gland enlargement, axillary hair loss, testicular atrophy, and peripheral neuropathy. Abdominal appearance of a cirrhotic patient with tense ascites.
Proximal muscles wasting in the setting of a hugely protuberant abdomen, prominent abdominal wall venous collaterals and small umbilical hernia.
Diagnosis
Routine laboratory tests of liver function may be normal in cirrhosis. Decreased serum albumin and a prolonged prothrombin time directly reflect impaired hepatic function. Transaminase is often modestly elevated, while alkaline phosphatase may be normal or increased, particularly with biliary obstruction. Bilirubin is usually normal. Anemia is fairly common and usually normocytic, but it may be microcytic, hypochromic from chronic GI bleeding, macrocytic from folate deficiency (in alcoholism), or hemolytic from hypersplenism. Alcohol directly suppresses the bone marrow. Hypersplenism also can lead to leukopenia and thrombocytopenia. Ultrasound may reveal textural abnormalities suggestive of cirrhosis, confirm hepatosplenomegaly, and detect features of portal hypertension: enlargement or obstruction of the portal or splenic veins and the presence of ascites, as well as the formation of HCC. CT better evaluates liver size and texture and, for hemochromatosis, density. Endoscopy is best for diagnosing esophageal varices.
- Liver cancer – etiology, pathogenesis, clinical presentation, diagnosis.
Abstract:
- hepatocellular carcinoma is a mostly malignant, solitary tumor of the liver
- often on basis of a liver cirrhosis/ chronic hepatitis
- often diagnoses as a incidental finding at sonography or higher alpha-fetoprotein
- clinical manifestation in the late stages in unspecific symptoms
- early stages: (part) resection of the liver or transplantation possible ● late stages: only palliative care
Etiology:
- 80% of the carcinomas are caused by liver cirrhosis
- chronic Hepatitis B or fatty liver
Symptoms:
- Early Stage: no specific symptoms
- Late Stage: unspecific symptoms in the upper abdominal region, weight loss, inappetite, icterus
- sometimes decompensated liver cirrhosis
Diagnostics:
- Laboratory: -AFP/alpha feto protein as a tumor marker
- Hepatitis laboratory parameters
- Imaging: – all contrast media imaging (sonography, MRT and CT)
- General: irregular vascularisation
- Sonography: different echos (in/homogenous)
- CT/MRT: for Staging and localisation in the liver
- CT Thorax: to look for lung metastases ● Punction: not in a curative therapy
Pathology:
- Histologic:
- (un)clear boarders tumor with capsula
- divers configurated tissue with trabecula
- neoplastic hepatocytes are a sign for malignancy ● Forms:
- fibrolamellar – solid
- Pseudoglandular – zirrhose
- pleomorphic – trabecular
- diffuse – clearcelled
Differential Diagnosis:
- Liver Metastases due to different other carcinomas
- Intrahepatic cholangiocellular carcinoma (CCC)
- Lymphoma of the liver
- Benign Liver Tumor (cyst, hyperplasia, adenoma, lipoma)
- Cholelithiasis and cholecystitis – etiology, pathogenesis, clinical presentation, diagnosis.
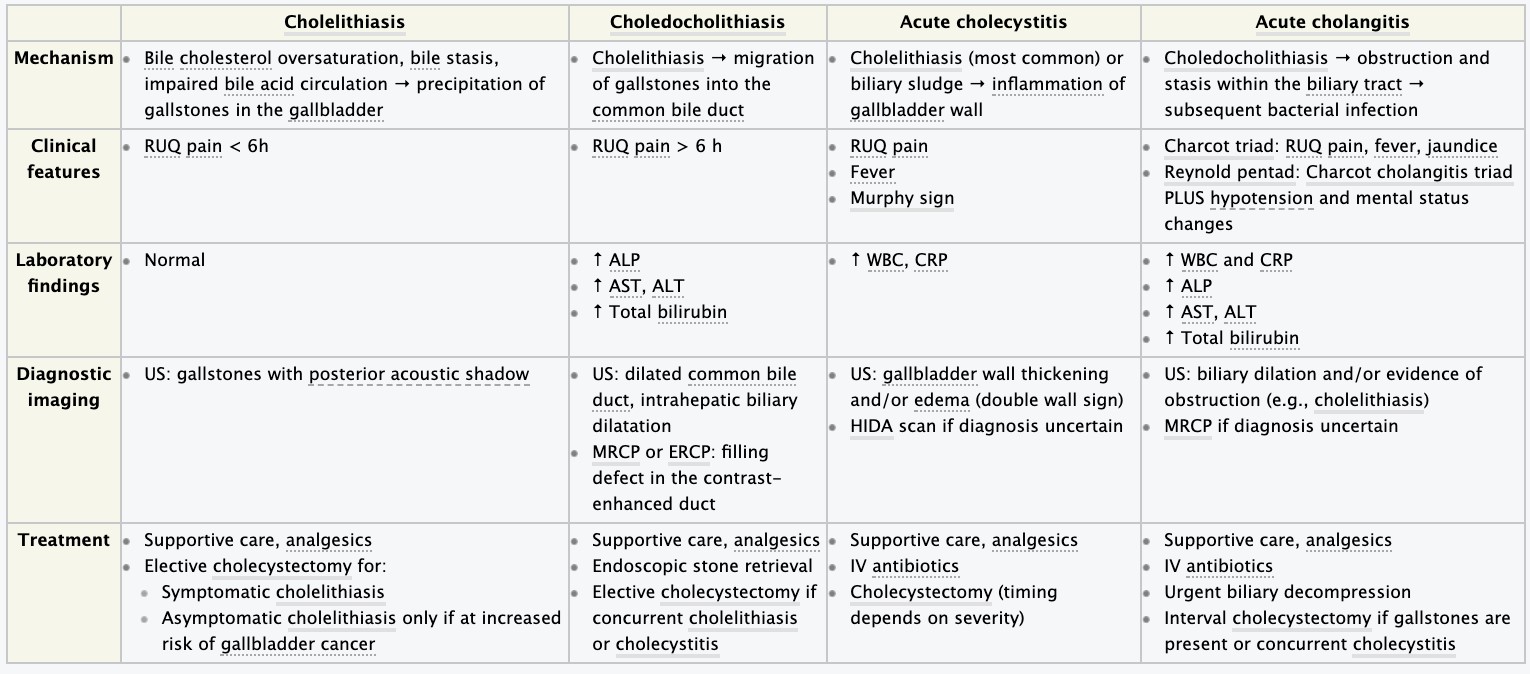
Cholelithiasis refers to the presence of gallstones in the gallbladder Epidemiology:
- Sex: ♀ > ♂ (2–3:1)
- Peak incidence: > 40 years Etiology
- Imbalance in bile salts, lecithin (stabilizer), cholesterol, calcium carbonate, and bilirubin ● Biliary stasis is a key component in gallstone formation.
- Impaired gallbladder emptying (e.g., due to bowel rest, prolonged total parenteral nutrition, pregnancy’G’q’>*%*$0&’”%#+M(’q’bile stasis (cholestasis)
| Cholesterol Stones (80% of all) | Black Pigment (10%) | Mixed(brown pig) (10%) |
| Risk factors
○ Obesity, Female sex ○ Age (> 40 years of age) ○ Multiparity or pregnancy ○ European, Native American, or Hispanic ancestry ○ Family history ○ Drugs: fibrates (inhibition of cholesterol 7-α hydroxylase), estrogen therapy, oral contraceptives ○ Malabsorption (e.g., Crohn disease, ileal resection, cystic fibrosis) Pathophysiologyo’$>,10=$%’ /(?$-*D’D/1%(“-(01%’=(-$>1%*”=’ q’V’D/1%(“-(01%’D1,D(,-0$-*1,’*,’ >*%(’$,+’W’>*%(’”$%-“’$,+’%(D*-/*,’ q’/&?(0″$-#0$-(+’>*%(’q’ ?0(D*?*-$-*1,’1C’D/1%(“-(01%’$,+’ D$%D*#=’D$0>1,$-(’q’D/1%(“-(01%’ “-1,(“’10’=*r(+’”-1,(“ | Risk factors
○ Chronic hemolytic anemias (e.g., sickle cell disease, hereditary spherocytosis) ○ Cirrhosis Pathophysiologyo’V’ /(=1%&”*”’q’*,D0($”(’*,’ D*0D#%$-*,M’#,D1,\#M$-(+’ >*%*0#>*,’q’*,D0($”(+’#?-$8(’ $,+’D1,\#M$-*1,’1C’>*%*0#>*,’ q’?0(D*?*-$-*1,’1C’>*%*0#>*,’ ?1%&=(0″’$,+’”-1,(’ C10=$-*1, | Risk factors: bacterial infections and parasites (e.g., Clonorchis sinensis, Opisthorcus species) in the biliary tract
Pathophysiologyo’*,C(D-*1,’10’ *,C(“-$-*1,’q’0(%($”(’1C’{9 M%#D#01,*+$”(’E>&’*,\#0(+’ /(?$-1D&-(“’$,+’>$D-(0*$G’q’ /&+01%&c(“’D1,\#M$-(+’ >*%*0#>*,’$,+’%(D*-/*,’*,’-/(’ >*%(’q’*,D0($”(+’ #,D1,\#M$-(+’>*%*0#>*,’$,+’ C$–&’$D*+”’q’?0(D*?*-$-*1,’1C’ D$%D*#=’D$0>1,$-(6’ D/1%(“-(01%6’$,+’D$%D*#=’ >*%*0#>*,$-(’E+$08’D1%10G’*,’ >*%( |
Clinical features:
- Most gallstones are asymptomatic.
- Biliary colic: constant, dull RUQ pain lasting < 6 hours
○ Especially postprandial
○ May radiate to the epigastrium, right shoulder, and back (referred pain)
- Nausea, vomiting, early satiety
- Bloating, dyspepsia Diagnosis:
➔ Approach: conduct RUQ’#%-0$”1#,+’q’?(0C10=’C#0-/(0’*=$M*,M’Es!R’10’MRCP) if concurrent common bile duct stones are suspected or if US is equivocal ➔ Laboratory findings: usually normal in uncomplicated cholelithiasis ➔ Imaging:
◆ RUQ ultrasound: best initial test (85–90% sensitivity, 99% specificity) [8]
-
- Shows gallstones with posterior acoustic shadow, possible sludge ◆ Endoscopic ultrasound (EUS) is more sensitive than transabdominal ultrasound. ◆ MRCP only if concurrent common bile duct stones are suspected Treatment:
- Supportive therapy: Fasting or dietary modification (decreased fat intake), Spasmolytics (e.g., dicyclomine), Analgesia: NSAIDs, opioids
- Surgical management: Laparoscopic cholecystectomy (curative) – Indications:
- Symptomatic cholelithiasis and Asymptomatic cholelithiasis with an increased risk of gallbladder cancer (e.g., gallbladder polyps or porcelain gallbladder present) – Timing: as soon as possible for biliary colic
- j(+*D$%’=$,$M(=(,-o’j(+*D$%’%*-/1%&”*”’E(:M:6’10$%’+*””1%#-*1,’-/(0$?&Go’10$%’
$+=*,*”-0$-*1,’1C’>*%(’$D*+”’ED/(,1+(1r&D/1%*D’$D*+6’#0″1+(1r&D/1%*D’$D*+G’^,+*D$-*1,o’
D/1%(“-(01%’”-1,(“’.*-/1#-’D$%D*C*D$-*1,’E2’LB’==G’C10’*,1?(0$>%(’?$-*(,-“’10’?$-*(,-“’./1’
+1’,1-’.*”/’-1’#,+(0M1’D/1%(D&”-(D-1=&:’f0($-=(,-’+#0$-*1,o’$-’%($”-’U’=1,-/”:’ R#DD(“”’0$-(’x’4B5
Complications:
-
- Gallstone ileus: mechanical ileus due to obstructive gallstones
○ Pathophysiology: perforation and fistula formation between the inflamed gallbladder’$,+’>1.(%’q’M$%%”-1,(“’?$””’+1.,’*,-1’>1.(%’%#=(,
○ Location: most commonly in the terminal ileum and ileocecal valve (intestinal section with the narrowest lumen)
○ Symptoms: abdominal pain and distention, nausea, vomiting
○ Typical signs: pneumobilia
- Gallstone pancreatitis
- Acute cholangitis
- Acute cholecystitis
- Biliary stricture
- Hepatic abscess (rare)
Cholecystitis is inflammation of the gallbladder that most commonly occurs after cystic duct obstruction from cholelithiasis. Acalculous cholecystitis is less common and seen primarily in critically ill patients.
Epidemiology:
- Sex: ♀ > ♂
- Prevalence: most common complication of cholelithiasis; occurs in up to 11% of patients with cholelithiasis
- Peak incidence: 40–50 years Etiology:
- Cause: obstructing cholelithiasis
- Pathophysiology: cholelithiasis’q’?$””$M(’1C’M$%%”-1,(“’*,-1’-/(’cystic duct’q’cystic duct’
1>”-0#D-*1,’q’+*”-(,-*1,’$,+’inflammation of the gallbladder
○ Bacterial infection may also be present (E. coli, Klebsiella, Enterobacter, Enterococcus spp. most common) but is not required for the development of cholecystitis. Clinical features:
- RUQ pain
○ More severe and prolonged (> 6 hours) than in cholelithiasis
○ Postprandial
○ Radiation to the right scapula
- Positive Murphy sign: sudden pausing during inspiration upon deep palpation of the right upper quadrant due to pain
- Guarding
- Fever, malaise, anorexia
- Nausea and vomiting Diagnosis:
- Laboratory findings
○ Elevated inflammatory markers (especially leukocytes and CRP) ○ Mild elevation in AST, ALT, amylase levels are possible.
○ Elevation in ALP, GGT, bilirubin levels are not common in uncomplicated cholecystitis and suggest biliary obstruction.
- Imaging
○ Transabdominal ultrasound
■ Gallbladder wall thickening > 4 mm (postprandial > 5 mm), Gallbladder wall edema (double wall sign), Possible free fluid surrounding the gallbladder
■ Sonographic Murphy sign, Presence of concrement or gallstones
○ HIDA scan (cholescintigraphy) if US is not diagnostic
■ Z$+*1$D-*)(’-0$D(0’ww=fD9/(?$-*D’*=*,1+*$D(-*D’$D*+’*”’*,\(D-(+’
*,-0$)(,1#”%&’q’”(%(D-*)(’#?-$8(’>&’hepatocytes’q’”#>”(u#(,-’(rD0(-*1,’
*,-1’bile’q’D$,’>(’)*”#$%*c(+’)*$’$’M$==$’D$=(0$
■ Abnormal if gallbladder not visualized within 30–60 minutes: suggests cystic duct obstruction due to edema or obstructing stone Treatment:
- Supportive therapy
○ Analgesia, Fluid and electrolyte correction, Antiemetics
- Intravenous antibiotics: Empiric antibiotic selection depends on individual and local factors (e.g., severity of infection, community-acquired vs. healthcare-associated infection, local resistance patterns)
- Surgical management
○ Cholecystectomy – Laparoscopic cholecystectomy is usually preferred. Complications
| acute cholecystitis | chronic cholecystitis | laparoscopic cholecystectomy |
of pus in the gallbladder
|
fibrotic and calcified gallbladder due to chronic inflammation
|
Bleeding
|
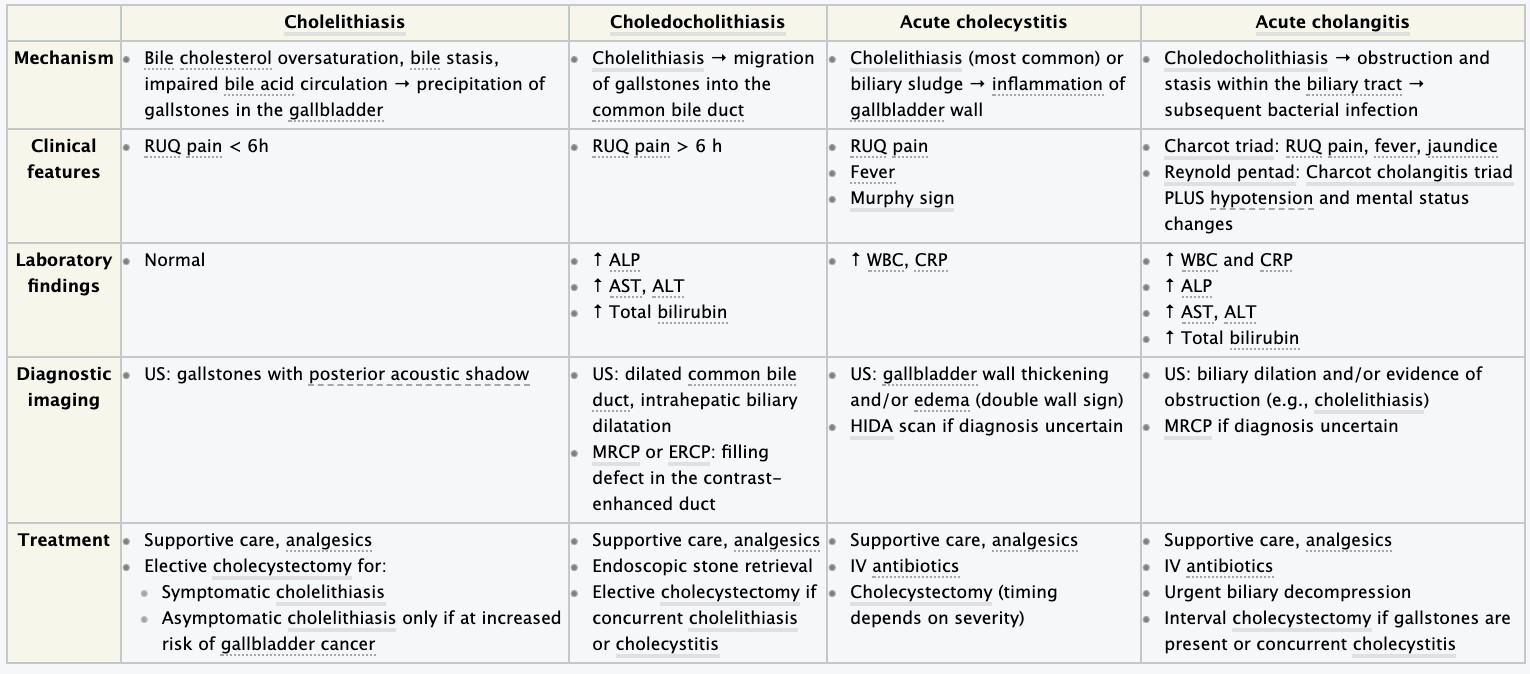
- Acute pancreatitis and chronic pancreatitis – etiology, pathogenesis, clinical presentation, diagnosis.
Pancreatitis is a condition characterized by inflammation of the pancreas.The pancreas is a large organ behind the stomach that produces digestive enzymes and a number of hormones.There are two main types: acute pancreatitis, and chronic pancreatitis.
^-’”1=(-*=(“’/($%”’.*-/1#-’$,&’*=?$*0=(,-’1C’C#,D-*1,’10’$,&’=10?/1%1M*D’D/$,M(“q’$D#-( pancreatitis (AP)
^-’D$,’0(D#0’*,-(0=*–(,-%&6’D1,-0*>#-*,M’-1’-/(’C#,D-*1,$%’$,+’’=10?/1%1M*D’%1″”’1C’-/(’M%$,+:’ Z(D#00(,-’$–$D8″’q’F/01,*D’?$,D0($-*-*”’EFdG
Acute Pancreatitis
The two types of acute pancreatitis are mild and severe, which are defined based on whether the predominant response to cell injury is inflammation (mild) or necrosis (severe). In mild pancreatitis, there is inflammation and edema of the pancreas. In severe pancreatitis, there is necrosis of the pancreas, and nearby organs may become injured.
Etiology
- Major causes: long standing alcohol consumption + biliary stone disease (cholelithiasis+ choledocholithiasis)
- Ethanol leads to intracellular accumulation of digestive enzymes & their premature activation release
1’s-/$,1%’V’?(0=($>*%*-&’1C’+#D-#%#”’$%%1.*,M’-/(’(,c&=(“’-1’0($D/’-/(’?$0(,D/&=$
1’s-/$,1%’V’-/(’?01-(*,’D1,-(,-’1C’-/(’?$,D0($-*D’\#*D(’>*D$0>1,$-(’%()(%”|’-0&?”*,’*,/*>*-10’D1,D:
This leads to formation of protein plugs that block the pancreatic outflow+ obstruction o A biliary stone may lodge in the pancreatic duct or ampulla of Vater leading to extravasation of enzymes into parenchyma
- Minor causes: medications, hypertriglyceridemia, peptic ulcer disease, trauma to abdomen/ back, pancreatic carcinoma, viral + bacterial infection, intestinal parasites, vascular factors
Pathogenesis of acute pancreatitis o Because its located in the retroperitoneal space with no capsule, inflammation can spread easily.
1’d$0(,D/&=$%’(+(=$’?(0*?$,D0($-*D’C$-’,(D01″*”’1DD#0″’C*0″-’q’$D#-(’(+(=$-1#”’?$,D0($-*-*”:’ e/(,’,(D01″*”’*,)1%)(“’-/(’?$0(,D/&=$6’$DD1=?$,*(“’>&’/$(=100/$M(’|’+&”C#,D-*1,’1C’-/(’ M%$,+6’*,C%$==$-*1,’()1%)(“’*,-1’/$(=100/$M*DN’,(D01-*”*,M’?$,D0($-*-*”
- Pseudocysts + pancreatic abscesses can result from necrotising pancreatitis because of the enzymes being walled off by granulation tissue (i.e. pseudocysts formation) or bacterial seeding of pancreatic/ peripancreatic tissue (1.e. pancreatic abscess formation) o An ultrasound/ preferably a CT scan can be used to detect both
1’^,C%$==$-*1,’?01D(“”’D$,’D$#”(’”&”-(=*D’(CC(D-“’+#(’-1’-/(’?0(“(,D(’1C’D&-18*,(“’E>0$+&8*,*,’
|’?/1″?/1%*?$”(’YG:’f/(“(’D$#”(’)$”1+*%$-*1,6’V’)$”D#%$0’?(0=($>*%*-&6’?$*,|’%(#81D&-(’
$DD#=#%$-*1,’*,’)(“”(%’.$%%”
1’[$-’,(D01″*”’q/&?1D$%D(=*$:’d$,D0($-*D’X’D(%%’*,\#0&’q/&?(0M%&D(=*$
Clinical Presentation of acute pancreatitis o Epigastric pain/ right upper quadrant pain
- Nausea +/ vomiting o Fever o Diarrhoea, indigestion jaundice o Tenderness/ swelling of tummy
Diagnosis of acute pancreatitis
- Blood test
- CT scan for confirmation o MRI+ ultrasound to determine severity o Ultrasound: diffuse enlargement, unclear contours, hypoechoic but homogenous structure. Complications: necrosis, pseudocysts, ascites, pleural effusions, abscess, splenic vein thrombosis with splenomegaly
Pathogenesis of chronic pancreatitis o Any theory concerning the pathophysiology of chronic pancreatitis must account for its well established morphologic features:
- Chronic inflammation
- Atrophy of secretory tissue
- Fibrosis
- Duct calculi in some cases o One theory:
y’S($)&’$%D1/1%’#”(’qD/$,M(’*,’D1=?1″*-*1,’1C’?$,D0($-*D’\#*D(’?0(D*?*-$-*1,’1C’?%#M”’E*,*-*$%%& in smaller pancreatic ducts) containing proteins+ calcium salts y’f/(“(’?%#M”’1>”-0#D-’-/(’+#D-“’q*,C%$==$-*1,6’C*>01″*”|’$-01?/&
§ According to this theory, CP is initially a ‘duct-based’ disease+ ultimately lead to ductal structure+ calculi o Alternative concept:
§ Result of either repetitive acute injury/ continuous subclinical injury produced by factors like alcohol consumption
§ Cell necrosis+ inflammation fibrosis+ atrophy+ secondary damage to ducts
§ This is the necrosis-fibrosis sequence+ is analogous to proposed theories describing the development of cirrhosis because of chronic hepatitis due to variety of causes
Clinical Presentation of chronic pancreatitis
- Repeated episodes of severe pain in abdomen, usually in middle/left side+ can move along your back. It’s described as burning/ shooting pain that comes and goes. o Poor digestion (malabsorption)
- Diabetes (1 in 3 cases as not enough insulin is produced) o Nausea
Diagnosis of chronic pancreatitis o Stool sample
- CT scan, endoscopic ultrasound scan
- MRCP o Biopsy
- Ultrasound: heterogenous, rough structure, irregularly dilated pancreatic duct, calcifications often found
97. Cancer of the pancreas – etiology, pathogenesis, clinical presentation, diagnosis.
Etiology mostly unclear
– suspected: genetic disposition, smoking, drinking, adipositas, chronic pancreatitis, and diabetes mellitus
Age is one of the greatest risk factors for pancreatic cancer with median age at diagnosis of 70 years. higher for males and blacks of both sexes.
Pathogenesis
Cancers of the pancreas can be divided into neoplasms of the endocrine pancreas and tumors of the exocrine pancreas. The most common neoplasm of the exocrine pancreas and most deadly is pancreatic infiltrating ductal adenocarcinoma. These tumors arise in the head, body, or tail of the pancreas and are characterized by infiltrating desmoplastic stromal reactions.
Other subtypes of non neuroendocrine pancreatic cancers include acinar cell carcinoma (tumors of the exocrine enzyme producing cell); medullary carcinoma, adenosquamous, and other rare subtypes. Each of these are different in their behaviors and in their molecular characteristics and often require specific other types of treatment.
Clinical presentation
The classic presentation for a patient with pancreatic cancer has been abdominal pain and weight loss with or without jaundice. The pain is midepigastric (sometimes described as a “boring-like” pain). Often the pain is in the back (due to retroperitoneal invasion of the splanchnic nerve plexus). The pain may be exacerbated by eating or lying flat. Other items of note in a history is lightening in stool color (steatorrhea also causes malodorous stools), or the onset of diabetes in the prior year. Jaundice, first detectable with a bilirubin of 2.5–3.0 mg/dL, is usually associated with tumor in the head of the pancreas. In some instances, depression is noted (with a higher subsequent number of suicides). Pruritus may be seen when the bilirubin reaches 6–8 mg/dL.
Physical signs include jaundice, signs of weight loss, a palpable gallbladder
(Courvoisier’s sign), hepatomegaly, an abdominal mass, and even an enlarged spleen (usually indicating a portal vein thrombosis). Migratory superficial thrombophlebitis can also be seen (Trousseau’s syndrome). Signs of late disease include a lymph node palpable in the supraclavicular fossa (usually on the left where the thoracic duct enters the subclavian vein). This is clinically referred to as Virchow’s node. Occasionally one can palpate subcutaneous metastases in the periumbilical area referred to as a Sister Mary Joseph’s node—named after one of the scrub nurses on the Mayo Clinic Operative Team who noted that when she prepped that area and felt those nodules, the patient often had peritoneal metastases.
Diagnosis
Diagnostic imaging plays a major role in diagnosing pancreatic cancer and other intraabdominal diseases. The best technique is the use of a dual-phase contrastenhanced spiral CT using the pancreatic cancer protocol which allows arterial phase enhancement and portal venous phase enhancement. This special protocol can provide helpful prospective staging and assessment of resectability. Figure 79-2 demonstrates such a CT scan (with vascular involvement). Figure 79-3 demonstrates the use of an 18F glucose positron emission tomography (PET) scan.
A histologic (tissue) diagnosis is essential and should be obtained with a cutting biopsy needle (not a skinny needle with cytology). Misdiagnosis is more common based on only fine-needle aspirates. Obtaining a tissue diagnosis allows not only for accuracy but also for molecular testing for KRAS mutations, microsatellite instability, and other important molecular abnormalities. Those molecular abnormalities and others will be increasingly important as more targeted therapies are developed for patients with pancreatic cancer.
The core needle (16–18 gauge) biopsy can be obtained via endoscopic ultrasoundguided techniques for a tumor localized to the pancreas or, if there are liver lesions or Virchow’s node, via percutaneous biopsy by interventional radiologists.
Serum Markers
Before treatment, a serum sample should be obtained for levels of CA19-9, carcinoembryonic antigen (CEA), or if both are negative, for CA125 (can be positive when the CA19-9 is negative due to the patient not being a Lewis antigen secretor). These markers are not useful for staging but can be useful in following the course of pancreatic cancer.
98. Chronic iron-deficiency anemia – etiology, pathogenesis, clinical presentation, diagnosis.
ETIOLOGY
Blood loss. Blood contains iron within red blood cells. So if you lose blood, you lose some iron. Women with heavy periods are at risk of iron deficiency anemia because they lose blood during menstruation. Slow, chronic blood loss within the body — such as from a peptic ulcer, a hiatal hernia, a colon polyp or colorectal cancer — can cause iron deficiency anemia. Gastrointestinal bleeding can result from regular use of some over-the-counter pain relievers, especially aspirin.
A lack of iron in your diet. Your body regularly gets iron from the foods you eat. If you consume too little iron, over time your body can become iron deficient. Examples of iron-rich foods include meat, eggs, leafy green vegetables and iron-fortified foods. For proper growth and development, infants and children need iron from their diets, too.
An inability to absorb iron. Iron from food is absorbed into your bloodstream in your small intestine. An intestinal disorder, such as celiac disease, which affects your intestine’s ability to absorb nutrients from digested food, can lead to iron deficiency anemia. If part of your small intestine has been bypassed or removed surgically, that may affect your ability to absorb iron and other nutrients.
Pregnancy. Without iron supplementation, iron deficiency anemia occurs in many pregnant women because their iron stores need to serve their own increased blood volume as well as be a source of hemoglobin for the growing fetus.
PATHOGENESIS
Iron deficiency anemia is a common type of anemia — a condition in which blood lacks adequate healthy red blood cells. Red blood cells carry oxygen to the body’s tissues. As the name implies, iron deficiency anemia is due to insufficient iron. Without enough iron, your body can’t produce enough of a substance in red blood cells that enables them to carry oxygen (hemoglobin). As a result, iron deficiency anemia may leave you tired and short of breath.
CLINICAL PRESENTATION
- Extreme fatigue
- Weakness
- Pale skin
- Chest pain, fast heartbeat or shortness of breath
- Headache, dizziness or lightheadedness
- Cold hands and feet
- Inflammation or soreness of your tongue
- Brittle nails
- Unusual cravings for non-nutritive substances, such as ice, dirt or starch
- Poor appetite, especially in infants and children with iron deficiency anemia
DIAGNOSIS
– full blood count (FBC) test
99. Vitamin B12 and folic acid- deficiency anemia – etiology, pathogenesis, clinical presentation, diagnosis.
Vitamin B12 or folate deficiency anaemia occurs when a lack of either of these vitamins affects the body’s ability to produce fully functioning red blood cells. Etiology:
Vitamin B-12 deficiency anemia
Plays an essential role in enzymatic reactions responsible for RBC formation and proper myelination of the nervous system.
Etiology:
- Malabsorption
○ W’Intrinsic factor
■ Pernicious anemia: most common cause of vitamin B12 deficiency
■ Atrophic gastritis (e.g., secondary to H. pylori infection)
■ Gastrectomy
○ W’Z(+#D(+’#?-$8(’1C’^[9vitamin B12 complex in terminal ileum: e.g., Crohn’s disease, celiac disease, pancreatic insufficiency, surgical resection of the ileum
- Malnutrition: e.g., chronic alcoholism, anorexia nervosa, or strict vegan diets
- Increased demand: e.g., during pregnancy, breastfeeding, fish tapeworm (Diphyllobothrium latum) infections, and leukemia Pathophysiology:
| Dysfunctional biochemical reactions | Pernicious anemia |
| Physiological function: Vitamin B12 is a watersoluble cofactor for enzymatic reactions of DNA synthesis (via methionine synthase) and oddchain fatty acid metabolism (via methylmalonyl CoA mutase). A deficiency of vitamin B12 leads to enzyme dysfunction.
Dysfunctional methionine synthase (normally converts homocysteine to methionine, thereby demethylating N5-methyl-THF to THF) ○ q’W’Tetrahydrofolate (THFG’q’W’DNA’ “&,-/(“*”’q’%$0M(6’,#D%($-(+’hematopoietic’ D(%%”6’*,D%#+*,M’=(M$%1>%$”-“’q’ =(M$%1>%$”-*D’?0(D#0″10″’#,+(0M1’ apoptosis/ phagocytosed by macrophages’ q’?$,D&-1?(,*$’E*,D%#+*,M’megaloblastic anemia) ○ q’W’Methionine’q’,(#01?$-/&’ ○ q’V’Homocysteine’q’(,+1-/(%*$%’+$=$M(’q’ ?0(+*”?1″(“’-1’D$0+*1)$”D#%$0’+*”($”( Dysfunctional methylmalonyl CoA mutase ○ Methylmalonyl CoA cannot be converted to succinyl CoA’q’$DD#=#%$-*1,’1C’ methylmalonyl CoA and its precursor propionyl CoA, as well as their associated odd-chain fatty acids, which cannot be completely metabolized ○ Propionyl CoA replaces acetyl CoA’*,’ ,(#01,$%’=(=>0$,(“’q’demyelination’q’ ,(#01%1M*D$%’=$,*C(“-$-*1, |
○ Antiparietal cell antibodies: target gastric parietal cells ■ F$#”(“’W’$D*+’?01+#D-*1,’$,+’ atrophic gastritis ■ W’Intrinsic factor’?01+#D-*1,’q’W’ vitamin B12 absorption in terminal ileum ○ Anti-IF antibodies: bind intrinsic factor and block the vitamin B12 binding site
diseases (e.g., hypothyroidism, vitiligo)
|
Clinical Symptoms:
- Signs of anemia (e.g., fatigue, pallor), Mild scleral icterus and/or jaundice
- Neurological disturbances : are generally symmetrical
- Peripheral neuropathy: tingling, numbness, pins-and-needles sensation, coldness (especially in the lower extremities)
- Subacute combined degeneration of spinal cord : symmetrical manifestations
- Loss of vibratory sensation, tactile discrimination, and proprioception
- Gait abnormalities (spinal ataxia, positive Romberg’s test) , Spastic paresis
- Neuropsychiatric disease (e.g., dementia, depression, paranoia), Worsening vision
- Autonomic dysfunction: impotence and incontinence, Glossitis Clinical Symptoms:
Signs of megaloblastic anemia
○ W’Hb
○ V’MCV (macrocyticG6’V’MCH (hyperchromic)
○ Hypersegmented neutrophils
○ W’Reticulocytes6’V’iron
Frequently thrombocytopenia and leukopenia (possibly pancytopenia)
Approach
If vitamin B12’”(0#=’%()(%”’$0(’+(D0($”(+’q’+(-(0=*,(’-/(’#,+(0%&*,M’D$#”(
- Test for autoantibodies
■ Anti-IF antibodies
■ Antiparietal cell antibodies
- If autoantibodies’$0(’,(M$-*)(’q’RD/*%%*,M’-(“-
■ Comprised of four stages that assess impaired vitamin B12 uptake
■ Stage 1: oral radiolabeled vitamin B12 + IM dose of unlabeled Vitamin B12
■ V’Z$+*1%$>(%(+’vitamin B12 in urine: Malnutrition or an increased demand is the most likely cause.
■ W’Z$+*1%$>(%(+’vitamin B12 in urine’q’?(0C10=’”-$M(’L
■ Stage 2: oral radiolabeled vitamin B12 + IF
■ V’Z$+*1%$>(%(+’vitamin B12 in urine: malabsorption due to lack of intrinsic factor
■ W’Z$+*1%$>(%(+’vitamin B12 in urine’q’?(0C10=’”-$M(’p
■ Stage 3: oral radiolabeled vitamin B12 + antibiotics
■ V’Z$+*1%$>(%(+’vitamin B12 in urine: bacterial overgrowth
■ W’Z$+*1%$>(%(+’vitamin B12 in urine’q’?(0C10=’”-$M(’_
■ Stage 4: oral radiolabeled vitamin B12 + pancreatic enzymes
■ V’Z$+*1%$>(%(+’vitamin B12 in urine: lack of pancreatic enzymes (e.g., chronic pancreatitis)
■ Gastroscopy
■ D-xylose absorption test
3. If vitamin B12 serum levels are normal q’j($”#0(’homocysteine: elevated in both vitamin B12 and folate deficiencies q’j($”#0(’jjY’-1’/(%?’0#%(’1#-’folate deficiency (normal MMA, elevated in B12 deficiency Treatment:
- IM supplementation of vitamin B12 (e.g., cyanocobalamin, hydroxocobalamin)
- Prevent future vitamin B12 deficiency by treating the underlying disease if possible (causative therapy): e.g., for fish tapeworm infestation, intestinal bacterial overgrowth, or chronic pancreatitis
Folate – deficiency anemia
Folate (vitamin B9) is an essential coenzyme that enables critical biochemical reactions – DNA synthesis and AA metabolism.The clinical picture of anemia is similar to that of vitamin B12 deficiency, although folate deficiency is generally not associated with neurological manifestations.
Etiology
- Malnutrition – “Tea and toast” diet, Alcohol use disorder
- Malabsorption: e.g., celiac disease, inflammatory bowel disease
- Increased requirement: e.g., pregnancy/lactation, severe hemolytic anemia ● Drug-related- Methotrexate, Antiepileptic drugs (e.g., phenytoin ), Trimethoprim Pathophysiology:
W’Folate’q’W’THF
- q’W’DNA’”&,-/(“*”’q’=(M$%1>%$”-*D’erythropoiesis’q’megaloblastic anemia’E|’W’*,’1-/(0’
D(%%’%*,(“G
- q’W’methionine’|’V’homocysteine’q’(,+1-/(%*$%’+$=$M(’Eq’V’0*”8’1C’D$0+*1)$”D#%$0’ +*”($”(’|’thromboembolic events)
- During fetal developmento’q’nucleotide’”&,-/(“*”’*=?$*0=(,-’q’neural tube defects 4. q’Y>(00$,-’DNA methylation’q’*,D0($”(+’0*”8’1C’D$,D(0’
Clinical features:
- Signs of anemia (e.g., fatigue, pallor)
- Sore tongue (glossitis ) Diagnostics:
- V’MCV (> 100 µm3)
- V’homocysteine
- Methylmalonic acid (MMA) is normal (unlike in vitamin B12’+(C*D*(,D&6’./(0(’jjY’*”’VG
- Hypersegmented neutrophils and pancytopenia may be present
- Folate serum levels are not reliable
Treatment: Oral folate supplementation for four months or until hematologic recovery takes place, Nutritional counseling to increase folate intake
100. Hemolytic anemia – etiology, pathogenesis, clinical presentation, diagnosis.
At the end of their normal life span (about 120 days), red blood cells (RBCs) are removed from the circulation. Hemolysis involves premature destruction and hence a shortened RBC life span (< 120 days). Anemia results when bone marrow production can no longer compensate for the shortened RBC survival; this condition is termed uncompensated hemolytic anemia. If the marrow can compensate, the condition is termed compensated hemolytic anemia.
Anaemia due to haemolysis, the abnormal breakdown of RBCs either in blood vessels (intravascular haemolysis) or elsewhere in the body (extravascular).
Classification: inherited/ acquired
Inherited: hemoglobinopathies (sickle cell disease thalassemia) enzymopathies, membranopathies
(hereditary spherocytosis) Etiology and Pathogenesis
F/$0$D-(0*”(+’>&’?0(=$-#0(’+(“-0#D-*1,’1C’ZXFR’V’*,’(0&-/01?1*(“*”’.*-/*,’-/(’>1,(’=$001.’
@10=1D&-*D’,10=1D/01=*D’ZXF6’V’0(-*D#%1D&-(“6’”?%(,1=(M$%&’\$#,+*D(
Acquired haemolytic anaemia: Haemolysis of RBC by
- Direct membrane destruction
- Ab mediated reaction caused by exogenous factors, drugs, chemicals, toxic venoms, mechanical factors like severe burns, prosthetic heart valves vasculitis
- Immune mediated reaction caused by Ab that damage that RBC membrane (transfusion reactions +haemolytic disease of the new-born) Inherited haemolytic anaemia:
- 2 main types of hemoglobinopathies can cause RBC haemolysis: Abnormal substitution of an amino acid in the haemoglobin molecule (Sickle cell)+ Defective synthesis of one of the polypeptide chains that form the globin portion of haemoglobin (Thalassemia)
- Sickle cells results from a point mutation in the beta chain of haemoglobin, with an abnormal substitution of a single AA, valine for glutamic acid
Clinical presentation
- Pale skin
- Dark urine
- Fever, weakness, dizziness, confusion
- Enlarged spleen/ liver
- Tachycardia
Diagnosis
Peripheral blood smear microscopy:
- Fragment of RBC ‘schistocytes’ can be present
- Some RBCs may appear smaller and rounder than usual (spherocytes) ● V’Z(-*D#%1D&-(“:’f/*”’=$&’>(’1)(0%118(+’*C’$’”?(D*$%’”-$*,’*”’,1-’#”(+: V’F1,\#M$-(+’>*%*0#>*,’*,’>%11+’\$#,+*D(
V’OgS
WS(=1M%1>*,’%()(%”
If the direct Coombs test is positive, haemolysis is caused by an immune process
Hemosiderin in urine indicates chronic intravascular haemolysis, no urobilinogen in urine
101. Polycythemia – clinical presentation, diagnosis.
Polycythemia (also known as polycythaemia or polyglobulia) is a disease state in which the hematocrit (the volume percentage of red blood cells in the blood) and/or hemoglobin concentration are elevated in peripheral blood.
Clinical presentation
- Tiredness (fatigue)
- Itching (especially after a warm shower)
- Headache
- Sweating (at night or during the day)
- Blurred vision or blind spots
- Painful burning or numbness of the hands or feet
- Bleeding from the gums and heavy bleeding from small cuts
- Bone pain
- Shortness of breath
- Abdominal pain or discomfort
- Early feeling of fullness when eating
- Pain under the left ribs
- Problems concentrating
- Dizziness, vertigo, lightheadedness
- Insomnia
- Reddening of the face, or a burning feeling on the skin
- Angina (chest pain)
- Ringing in the ears
Diagnosis
Blood tests
If you have polycythemia vera, blood tests might reveal:
- More red blood cells than normal and, sometimes, an increase in platelets or white blood cells
- A greater percentage of red blood cells that make up total blood volume
(hematocrit measurement)
- Elevated levels of the iron-rich protein in red blood cells that carries oxygen (hemoglobin)
- Very low levels of a hormone that stimulates bone marrow to produce new red blood cells (erythropoietin)
Bone marrow aspiration or biopsy
If your doctor suspects that you have polycythemia vera, he or she might recommend collecting a sample of your bone marrow through a bone marrow aspiration or biopsy.
A bone marrow biopsy involves taking a sample of solid bone marrow material. A bone marrow aspiration is usually done at the same time. During an aspiration, your doctor withdraws a sample of the liquid portion of your marrow.
Specific gene testing
If you have polycythemia vera, analysis of your bone marrow or blood might show the gene mutation that’s associated with the disease.
102. Acute leukemia – etiology, pathogenesis, clinical, hematological forms, diagnosis.
Leukemia is a cancer of the blood or bone marrow. Bone marrow produces blood cells. Leukemia can develop due to a problem with blood cell production. It usually affects the leukocytes, or white blood cells.
ETIOLOGY
No one knows exactly what causes leukemia. People who have it have certain unusual chromosomes, but the chromosomes don’t cause leukemia.
You can’t prevent leukemia, but certain things may trigger it. You might have a higher risk if you:
- Smoke
- Are exposed to a lot of radiation or certain chemicals
- Had radiation therapy or chemotherapy to treat cancer
- Have a family history of leukemia
- Have a genetic disorder like Down syndrome
PATHOGENESIS
Leukemia develops when the DNA of developing blood cells, mainly white cells, incurs damage. This causes the blood cells to grow and divide uncontrollably. Healthy blood cells die, and new cells replace them. These develop in the bone marrow. The abnormal blood cells do not die at a natural point in their life cycle. Instead, they build up and occupy more space. As the bone marrow produces more cancer cells, they begin to overcrowd the blood, preventing the healthy white blood cells from growing and functioning normally. Eventually, the cancerous cells outnumber healthy cells in the blood.
CLINICAL PRESENTATION
- Weakness or fatigue
- Bruising or bleeding easily
- Poor blood clotting
- Frequent infections
- anemia
- Fever or chills
- Infections that are severe or keep coming back
- Pain in bones or joints
- Headaches
- Vomiting
- Seizures
- Weight loss
- Night sweats
- Shortness of breath
- Swollen lymph nodes or organs like the spleen
HEMATOLOGICAL FORMS
There are four main categories of leukemia:
- acute
- chronic
- lymphocytic
- myelogenous
The first group, how fast it develops, is divided into acute and chronic leukemia.
- Acute leukemia happens when most of the abnormal blood cells don’t mature and can’t carry out normal functions. It can get bad very fast.
- Chronic leukemia happens when there are some immature cells, but others are normal and can work the way they should. It gets bad more slowly than acute forms do
The second group, what type of cell is involved, is divided into lymphocytic and myelogenous leukemia.
- Lymphocytic (or lymphoblastic) leukemia involves bone marrow cells that become lymphocytes, a kind of white blood cell.
- Myelogenous (or myeloid) leukemia involves the marrow cells that create red blood cells, platelets, and other kinds of white blood cells.
DIAGNOSIS
- Blood tests
- Bone marrow biopsy
- Spinal tap
- Imaging tests – CT, MRI, PET
103. Chronic myeloid leukemia – etiology, pathogenesis, clinical and hematologic presentation, diagnosis.
CML is a cancer of white blood cells that is characterised by uncontrolled growth of myeloid cells in the bone marrow.
- This uncontrolled growth leads to myeloid cells crowding out the bone marrow and interfering with the production of normal blood cells such as platelets, erythrocytes and neutrophils.
- In addition to crowding out the bone marrow, the abnormal myeloid cells spill into the peripheral blood. This is reflected in the full blood count which demonstrates abnormally raised levels of mature granulocytes (neutrophils, basophils and eosinophils).
Etiology: CML was the first malignancy to be linked directly to a clear chromosomal abnormality.
- This abnormality involves a translocation between parts of chromosome 9 and 22, which leads to the formation of the so-called Philadelphia chromosome.
- As a result, a gene contained on chromosome 22 called BCR fuses with a gene on chromosome 9 known as ABL. This creates a hybrid gene known as BCR-ABL.
- This gene is able to add phosphates to tyrosine residues (a tyrosine kinase) and this allows BCR-ABL to activate a cascade of proteins which control the cell cycle, speeding up cell division.
- In addition, the BCR-ABL protein inhibits DNA repair, causing genomic instability and making the cell more susceptible to developing further genetic abnormalities. These two mechanisms of both speeding cell division and inhibiting DNA repair lead to chronic myeloid leukaemia. Clinical symptoms:
Often asymptomatic’9’?0(“(,-*,M’.*-/’V’./*-(’>%11+’D(%%’D1#,-’1,’01#-*,(’%$>10$-10&’-(“-*,M:
Symptoms of CML can include:
- Upper abdominal pain – hepatosplenomegaly
- Poor appetite – an enlarged spleen may compress the stomach
- Low-grade fever/night sweats (“B symptoms”)
- h1#-’‘’*,D0($”(+’D(%%’-#0,1)(0’q’(rD(“”’?#0*,(“’q’>018(,’+1.,’-1’#0*D’$D*+
- ^,D0($”(+’”#”D(?-*>*%*-&’-1’*,C(D-*1,”’‘’W’C#,D-*1,$%’*==#,(’D(%%”
- Shortness of breath/fatigue – anaemia
- Easy bruising/petechiae/bleeding – low platelets
- Neurological deficits/visual disturbance – hyperviscosity due to leukocytosis Phases:
- Chronic phase
- Approximately 85% of patients with CML are in the chronic phase at the time of diagnosis.
- During this phase, patients are asymptomatic or have only mild symptoms of fatigue or abdominal fullness.
- The duration is variable and without treatment, the disease progresses to the accelerated phase eventually (due to the accumulation of genetic mutations in addition to the BCRABL gene).
- Accelerated phase
- 10 – 19% myeloblasts in the blood or bone marrow
- >20% basophils in the blood or bone marrow
- Platelet count <100,000, unrelated to therapy
- Platelet count >1,000,000, unresponsive to therapy
- Cytogenetic evolution with new abnormalities in addition to the Philadelphia chromosome
- Increasing splenomegaly or white blood cell count, unresponsive to therapy
This phase is significant as it is a sign that the disease is progressing and that a blast crisis is imminent.
- Blast crisis
The final phase and behaves like acute leukaemia, with rapid progression and short survival.
- >20% myeloblasts or lymphoblasts in the blood or bone marrow
- Large clusters of blasts in the bone marrow on biopsy
- Development of a chloroma (a solid focus of leukaemia outside the bone marrow)
Diagnosis
Full blood count:
- Leukocytosis
- Increased numbers of eosinophils and basophils
- Differential WCC shows granulocytes at all stages of development
- Anaemia (normocytic/normochromic)
Biochemistry
- Lactate dehydrogenase is often raised
- Urate may be raised (due to high cell turnover)
- U&Es are usually normal at presentation
Bone marrow aspirate
- To stage disease (% of blasts determines chronic vs accelerated vs blast crisis)
- Allows cytogenetic sampling to confirm diagnosis – Philadelphia chromosome
- The gold standard of diagnosis is the detection of the Philadelphia chromosome, which is present in 95% of people with CML. Methods for identifying the Philadelphia chromosome include
◆ FISH (fluorescent in-situ hybridisation) and PCR for the BCR-ABL gene Treatment: management of disease with Tyrosine Kinase Inhibitors (TKI) and bone marrow transplant
104. Chronic lymphoid leukemia – etiology, pathogenesis, clinical and hematologic picture diagnosis.
CLL is a type of cancer of the blood + bone marrow
- Most commonly affects older adults
- Most tumour cells are small round lymphocytes; condensed chromatin scant cytoplasm.
- g*”0#?-(+’-#=1#0’D(%%”’E”=#+M(’D(%%”G’qD/$0$D-(0*”-*D’C*,+*,M
Chronic lymphocytic leukemia (CLL) belongs to the group of low-grade non-Hodgkin lymphomas (NHL) and is a B-cell lymphoma that presents with lymphocytic leukocytosis. CLL is the most common form of leukemia in adults and is typically considered a disease of the elderly. Clinical features include painless lymphadenopathy, fatigue, chronic pruritus, and an increased susceptibility to infections. Important diagnostic markers are smudge cells (Gumprecht shadows) in a blood smear, a high percentage of small, mature lymphocytes in the bone marrow, and detection of B-CLL antigens in flow cytometry.
Etiology and Pathogenesis
h(,(-*D’=#-$-*1,’*,’g@Y’1C’>%11+9?01+#D*,M’D(%%”’q$>,10=$%6’*,(CC(D-*)(’%&=?/1D&-(“’ qD1,-*,#(’-1’%*)(|’=#%-*?%&
They accumulate in blood+ certain organ where they cause complications
They may crowd healthy cells out of the bone marrow interfere with normal B3C production Exact mechanism not clear
Risk factors: age (70s), race (whites more likely), family history of blood+ bone married cancers, exposure to chemicals (herbicides, insecticides, Agent Orange used in Vietnam war)
Clinical presentation
- Enlarged, but painless lymph nodes
- Pain in the upper left portion of the abdomen, which may be caused by an enlarged spleen
- Fatigue, fever, night sweats
- Weight loss
- Frequent infections
Diagnosis
- X%11+’-(“-“o’FXF6’V’X’D(%%”
CBC
Persistent lymphocytosis with a high percentage of small mature lymphocytes Findings that indicate suppression of normal myelopoiesis:
Granulocytopenia
Low RBC count (due to autoimmune hemolysis) Low platelet count
- F&-1=(-0&N’*==#,1?/(,1-&?*,M’/(%?”’+(-(0=*,(’./(-/(0’$,V%&=?/1D&-(“’*”’+#(’-1’ FOO6’$’+*CC(0(,-’>%11+’+*”10+(0N’&1#0’>1+&}”’0($D-*1,’-1’$,1-/(0’?01D(“”:
- Analyse for genetic abnormalities: FISH (fluorescence in situ hybridisation)
105. Agranulocytosis and pancytopenia – etiology, pathogenesis, clinical and hematologic presentation diagnosis.
Agranulocytosis
Heavy depletion of granulocytes (WBC) in the peripheral blood (<500/<200ul). People with this condition are at very high risk of serious infections due to their suppressed immune system.
In agranulocytosis, the concentration of granulocytes (a major class of white blood cells that includes neutrophils, basophils, and eosinophils) drops below 200 cells/mm³ of blood. Etiology
Large number of drugs have been associated with agranulocytosis, including antiepileptics (such as carbamazepine and valproate), antithyroid drugs (carbimazole, thiamazole, and propylthiouracil), antibiotics (penicillin, chloramphenicol and cotrimoxazole), H2 blockers (cimetidine, famotidine, nizatidine, ranitidine, ACE inhibitors
(benazepril), cytotoxic drugs, gold, analgesics (aminophenazone, indomethacin, naproxen, phenylbutazone, metamizole), mebendazole, allopurinol the antidepressants mianserin and mirtazapine, and some antipsychotics (the atypical antipsychotic clozapine in particular). Clozapine users in the United States, Australia, Canada, and the UK must be nationally registered for monitoring of low WBC and absolute neutrophil counts (ANC).
The Centers for Disease Control traced outbreaks of agranulocytosis among cocaine users to be elevated.
- Chemotherapy to treat cancer.
- The use of some prescription drugs, particularly certain antibiotics, and antithyroid and anti-psychotic medications.
- Exposure to toxic substances, such as arsenic or mercury.
- Bone marrow failure disorders such as aplastic anemia.
- Other medical conditions, such as tumors or some autoimmune diseases.
Pathogenesis
In a general sense the pathogenesis of neutropenia can be divided into two categories;
- Inadequate or ineffective formation of granulocytes. This can be due to bone marrow failure such that occurs in aplastic anaemia, several leukaemias and chemotherapeutic agents. There can also be isolated neutropenias where only differentiated granulocyte precursors are affected as in the case of neoplastic proliferation of cytotoxic T cells or NK cells
- Accelerated destruction of neutrophils. Immune-mediated reactions to neutrophils which can be caused by drugs. An enlarged spleen can lead to splenic sequestration and accelerated removal of neutrophils. Utilization of neutrophils can occur in infections[9]
Clinical presentation
Agranulocytosis may be asymptomatic, or may clinically present with sudden fever, rigors and sore throat. Infection of any organ may be rapidly progressive (e.g., pneumonia, urinary tract infection). Sepsis may also progress rapidly.
Diagnosis
The diagnosis is made after a complete blood count, a routine blood test. The absolute neutrophil count in this test will be below 500, and can reach 0 cells/mm³. Other kinds of blood cells are typically present in normal numbers.
To formally diagnose agranulocytosis, other pathologies with a similar presentation must be excluded, such as aplastic anemia, paroxysmal nocturnal hemoglobinuria, myelodysplasia and leukemias. This requires a bone marrow examination that shows normocellular (normal amounts and types of cells) blood marrow with underdeveloped promyelocytes. These underdeveloped promyelocytes, if fully matured, would have been the missing granulocytes.
The following terms can be used to specify the type of granulocyte referenced:
- Inadequate numbers of neutrophils: neutropenia (most common)
- Inadequate numbers of eosinophils: eosinopenia (uncommon) ● Inadequate numbers of basophils: basopenia (very rare)
Pancytopenia is a condition in which a person’s body has too few red blood cells, white blood cells, and platelets. Each of these blood cell types has a different job in the body: Red blood cells carry oxygen throughout your body. White blood cells are part of your immune system and help fight off infection
Causes
Pancytopenia is usually due to some disruption of the bone marrow’s ability to produce new blood cells. Examples could include:
- cancer that destroys the bone marrow cells
- failure to make stem cells that turn into blood cells
- fibrosis or scarring of bone marrow cells
- immune system destroying healthy bone marrow cells
- suppression of bone marrow function due to illness or medications
Some of the conditions that can cause pancytopenia include:
- aplastic anemia
- autoimmune conditions
- cancer
- chemotherapy treatments
- exposure to toxins or pollutants, such as radiation or arsenic
- Fanconi’s anemia
- infection
- leukemia, which impacts bone marrow function
- megaloblastic anemia
- lupus
- deficiency of folate or vitamin B12 for making bone marrow
- taking medications that affect bone marrow function
- viruses, such as Epstein-Barr, HIV or hepatitis C
Medications that can affect bone marrow function include chloramphenicol, chemotherapy drugs, thiazide diuretics, anti-epileptic drugs, colchicine, azathioprine, and non-steroidal anti-inflammatory drugs (NSAIDs).
Pathogenesis
The mechanisms for pancytopenia differ according to the etiology. For example, in hemophagocytic lymphohistiocytosis (HLH) there is marked inappropriate and ineffective T cell activation that leads to an increased hemophagocytic activity. The T cell activated macrophages engulf erythrocytes, leukocytes, platelets, as well as their progenitor cells. Along with pancytopenia, HLH is characterized by fever, splenomegaly, and hemophagocytosis in bone marrow, liver, or lymph nodes.
Clinical manifestations
For example, red blood cells carry oxygen. Therefore, if a person does not have enough red blood cells due to pancytopenia, they may have difficulty breathing and feel fatigued.
Platelets are responsible for helping blood to clot, during wound healing. If a person’s platelets are low, they may bleed more easily.
White blood cells help to fight infection. Therefore, if a person has a low white blood cell count, they may be more prone to infection.
Additional symptoms associated with pancytopenia include:
- easy bleeding, such as from gums or nose
- easy bruising
- fast heart rate
- pale skin color
- rashes
- unexplained fatigue
- weakness
A person should go or be taken to the emergency room immediately if they have the following symptoms, all of which can occur suddenly:
- confusion
- loss of consciousness
- seizures
- shortness of breath
- significant blood loss
Diagnosis
A doctor will typically diagnose pancytopenia by ordering what is known as a complete blood count or CBC. This blood test gives values of red blood cells, white blood cells, and platelets.
A doctor may also order other laboratory tests, such as liver function tests, vitamin B-12 levels, HIV and hepatitis testing.
As well as laboratory testing, a doctor will also consider a person’s symptoms related to pancytopenia.
They may perform a procedure to sample a person’s bone marrow. A sample of bone marrow is commonly taken from the hip after the area has been numbed.
The sample is sent to a laboratory where a doctor will examine the cells under a microscope. The cells’ appearances can help identify the potential underlying cause of pancytopenia.
106. Bleeding disorders, types – etiology, pathogenesis.
TYPES
There are numerous different bleeding disorders, but the following are the most common ones:
- Hemophilia A and B are conditions that occur when there are low levels of clotting factors in your blood. It causes heavy or unusual bleeding into the joints. Though hemophilia is rare, it can have life-threatening complications.
- Factor II, V, VII, X, or XII deficiencies are bleeding disorders related to blood clotting problems or abnormal bleeding problems.
- Von Willebrand’s disease is the most common inherited bleeding disorder. It develops when the blood lacks von Willebrand factor, which helps the blood to clot.
ETIOLOGY
A bleeding disorder is a condition that affects the way your blood normally clots. The clotting process, also known as coagulation, changes blood from a liquid to a solid. When you’re injured, your blood normally begins to clot to prevent a massive loss of blood. Sometimes, certain conditions prevent blood from clotting properly, which can result in heavy or prolonged bleeding. Bleeding disorders can cause abnormal bleeding both outside and inside the body.
Some disorders can drastically increase the amount of blood leaving your body. Others cause bleeding to occur under the skin or in vital organs, such as the brain. The majority of bleeding disorders are inherited, which means they’re passed from a parent to their child. However, some disorders may develop as a result of other medical conditions, such as liver disease.
Bleeding disorders may also be caused by:
- a low red blood cell count
- a vitamin K deficiency
- side effects from certain medications
Medications that can interfere with the clotting of the blood are called anticoagulants.
PATHOGENESIS
Bleeding disorders often develop when the blood can’t clot properly. For blood to clot, your body needs blood proteins called clotting factors and blood cells called platelets. Normally, platelets clump together to form a plug at the site of a damaged or injured blood vessel. The clotting factors then come together to form a fibrin clot. This keeps the platelets in place and prevents blood from flowing out of the blood vessel.
In people with bleeding disorders, however, the clotting factors or platelets don’t work the way they should or are in short supply. When the blood doesn’t clot, excessive or prolonged bleeding can occur. It can also lead to spontaneous or sudden bleeding in the muscles, joints, or other parts of the body.
107. Hodgkin Disease. Non-Hodgkin lymphomas- etiology, pathogenesis, clinical and hematologic picture diagnosis.
Hodgkin’s lymphoma (HL) is a malignancy of mature B lymphocytes.
- It represents ~10% of all lymphomas diagnosed each year.
- The majority of HL diagnoses are classical HL (cHL), but there is a second subtype of HL, nodular lymphocyte predominant HL (NLPHL).
- 4 subtypes of cHL that are differentiated based on their histopathologic features:
A. nodular sclerosis – most common
B. mixed cellularity,
C. lymphocyte-rich,
D. lymphocyte-depleted.
Epidemiology
- Elderly patients, patients infected with HIV, and patients in Third World tend to have mixed cullairty and lymphocyte depleted HL
- Younger people tend to have nodular sclerosing
- Male predominance, especially in pediatric cases
Etiology: The exact causes are unknown, several risk factors associated with HL:
- Strong association with Epstein-Barr virus (EBV)
- Immunodeficiency: organ/ cell transplantation, immunosuppressants, HIV, chemotherapy ● Autoimmune diseases (e.g., rheumatoid arthritis, sarcoidosis) Clinical Symptoms:
- Painless lymphadenopathy
- Cervical lymph nodes’E*,’b’UB‘7B5’1C’?$-*(,-“G’v’axillary lymph nodes’E*,’b’L4‘p45’1C’
?$-*(,-“G’v’inguinal lymph nodes’E*,’b’3‘K45’1C’?$-*(,-“G’
○ Mediastinal mass’q’chest pain, dry cough, and shortness of breath
○ Splenomegaly or hepatomegaly may occur if the spleen or liver are involved.
- B symptoms
- Night sweats, weight loss > 10% in the past 6 months, fever > 38°C (100.4°F)
○ Can occur in a variety of diseases, such as non-Hodgkin lymphoma, other malignancies, tuberculosis, and various inflammatory diseases
○ The presence of only one of the symptoms – in the case of confirmed HL – is considered positive for B symptoms.
 Others: Pel-Ebstein fever, Alcohol-induced pain, Pruritus (focal or generalized) Staging is based on the number of affected nodes, the presence or absence of B symptoms, and whether or not the disease is present on both sides of the diaphragm.
Others: Pel-Ebstein fever, Alcohol-induced pain, Pruritus (focal or generalized) Staging is based on the number of affected nodes, the presence or absence of B symptoms, and whether or not the disease is present on both sides of the diaphragm.
Diagnosis: primarily with medical history, clinical symptoms and confirmed with lymph node biopsy
- X%11+’-(“-o’m
K:’F1=?%(-(’>%11+’D1#,-o’V10W’eXF’D1#,-6’$,(=*$6’(1″*,1?/*%*$m
L:’R(0#=’D/(=*”-0&o’VOgS6’/&?(0D$%D(=*$
- Histology (obligatory): Reed-Sternberg cells (pathologic), inflammatory cells, granulomas
- Radiology: Chest x-ray/CT-scan: detection and measurement of masses and enlarged lymph nodes in chest, abdomen, and pelvis Treatment:
- Early stage (I and II): combination of chemotherapy (ABVD) and radiation therapy
- Advanced stage (III and IV and often II with bulky disease): combination chemotherapy with radiation therapy in select cases. Possible approaches:
■ ABVD
■ Stanford V
■ BEACOPP
- Primary refractory or relapsed disease: trial of alternative chemotherapy or consideration of high-dose chemotherapy and autologous stem cell transplantation
Non-Hodgkin’s lymphomas (NHL)
Are cancers of mature B, T, and NK cells. Distinguished from HL upon recognition of the ReedSternberg (RS) cell, and differ with respect to their biologic and clinical characteristics.
- classified according to the cell type, i.e., B cells, T cells, and natural killer (NK) cells, and tumor grade.
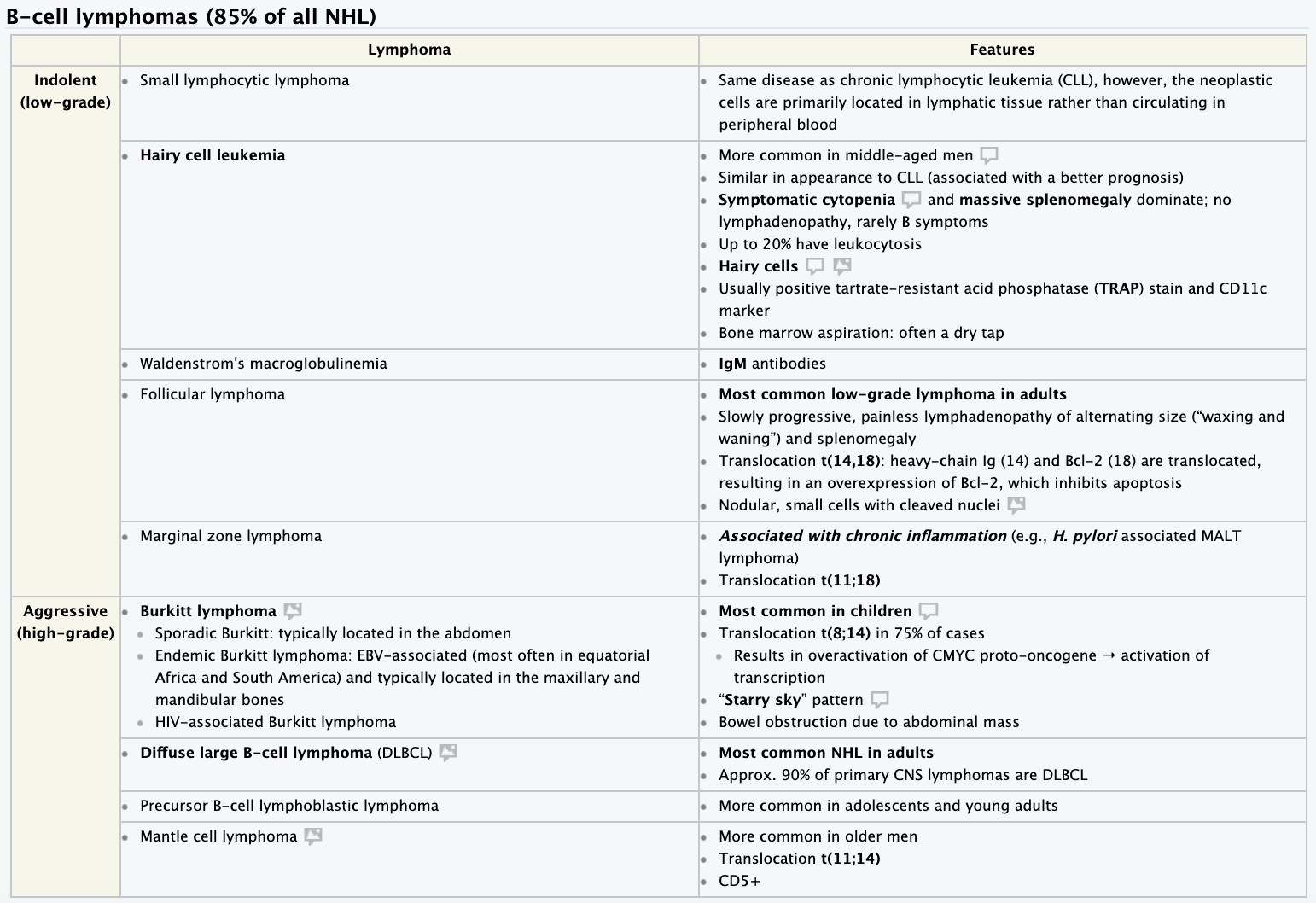 Low-grade tumors originate from mature cells with slow growth rate and an clinical course. The most common low-grade B-cell lymphoma is follicular lymphoma, while the most common low-grade T-cell lymphomas are the cutaneous T-cell lymphomas such as mycosis fungoides.
Low-grade tumors originate from mature cells with slow growth rate and an clinical course. The most common low-grade B-cell lymphoma is follicular lymphoma, while the most common low-grade T-cell lymphomas are the cutaneous T-cell lymphomas such as mycosis fungoides.- High-grade tumors have a rapid growth rate and an aggressive clinical course. Epidemiology:
- Most common hematopoietic neoplasm and compromises 85% of lymphomas
- Incidence of all NHL increases with age; peak incidence > 50 years
- High-grade lymphomas more common in children and young adults (20–40 years) Etiology:
- Chromosomal translocations: most commonly t(14;18)
- Infections: EBV, HIV, HTLV-1, HCV, Helicobacter pylori (gastric lymphoma)
- Autoimmune diseases: Hashimoto thyroiditis, rheumatic disease
- Immunodeficiency: congenital immunodeficiencies, AIDS, history of chemotherapy and/or immunosuppressive therapy
- Environmental factors: aromatic hydrocarbons (e.g., benzene), radiation
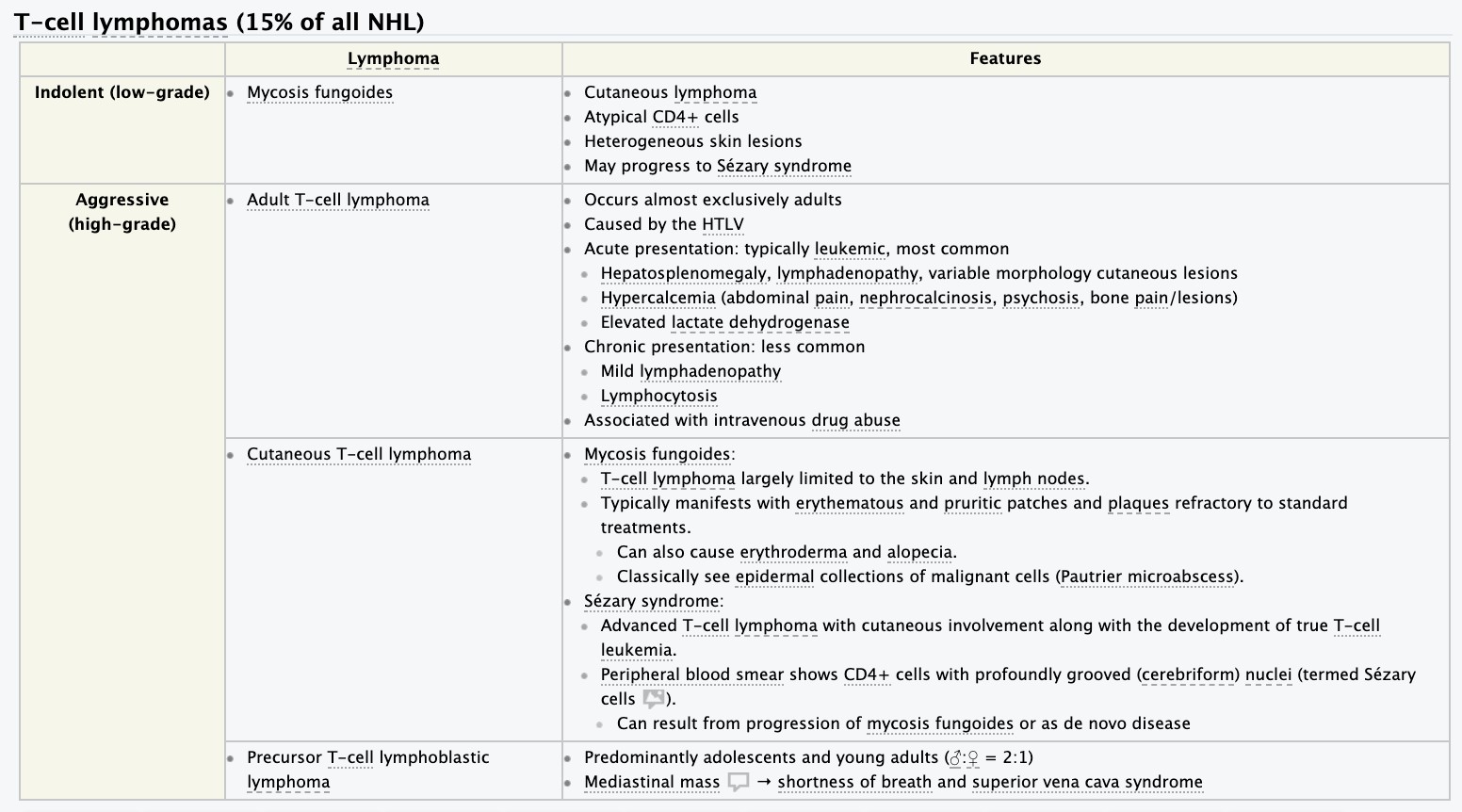
Clinical symptoms:
Insidious onset in low-grade lymphomas, Painless lymphadenopathy, Splenomegaly, hepatomegaly, Extranodal disease: most commonly involves the gastrointestinal tract, skin, thyroid, and CNS, B symptoms (weight loss, fever, night sweats), Fatigue, weakness, and signs of bone marrow involvement (anemia, bleeding, increased susceptibility to infections) Diagnosis: confirm with needle biopsy, similar tests to HL – blood tests, Histology (NO ReedSternberg cells), imagine – X-ray and CT for staging, immunohistochemistry, lumbar puncture. Treatment:
Some exceptions to the table:
- Primary CNS lymphoma:
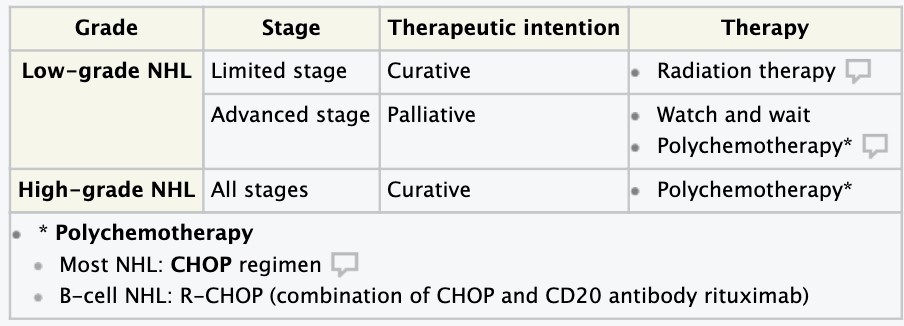 intrathecal methotrexate plus chemotherapy and/or radiation therapy plus dexamethasone
intrathecal methotrexate plus chemotherapy and/or radiation therapy plus dexamethasone
- Hairy cell leukemia: chemotherapy with cladribine or pentostatin
- Burkitt lymphoma: similar to acute lymphocytic leukemia
108. Multiple myeloma- etiology, pathogenesis, clinical and hematological picture
Multiple myeloma (MM), also known as plasma cell myeloma, Kahler’s disease,
myelomatosis and simple myeloma, is a cancer of plasma cells, a type of white blood cell that normally produces antibodies.Multiple myeloma may develop from monoclonal gammopathy of undetermined significance that progresses to smoldering myeloma. The abnormal plasma cells produce abnormal antibodies, which can cause kidney problems and overly thick blood The plasma cells can also form a mass in the bone marrow or soft tissue. When one tumor is present, it is called a plasmacytoma; more than one is called multiple myeloma
Etiology
The cause of multiple myeloma is generally unknown.
Risk factors
- Monoclonal gammopathy of undetermined significance (MGUS) increases the risk of developing multiple myeloma. MGUS transforms to multiple myeloma at the rate of 1% to 2% per year, and almost all cases of multiple myeloma are preceded by MGUS ● Smoldering multiple myeloma increases the risk of developing multiple myeloma. Individuals diagnosed with this premalignant disorder develop multiple myeloma at a rate of 10% per year for the first 5 years, 3% per year for the next 5 years, and then 1% per year.
- Obesity is related to multiple myeloma with each increase of body mass index by five increasing the risk by 11%.
Pathophysiology
Neoplastic proliferation of plasma cells
X1,(’=$001.’*,C*%-0$-*1,’q’”#??0(“”*1,’1C’/(=$-1?1*(“*”’q’%(#81?(,*$6’
-/01=>1D&-1?(,*$6’$,(=*$
F(%%’?01%*C(0$-*1,’q’1″-(1%&”*”’q’/&?(0D$%D(=*$
Overproduction of monoclonal immunoglobulin and/or light chains
@1,9C#,D-*1,*,M’$,-*>1+*(“’q’C#,D-*1,$%’$,-*>1+&’+(C*D*(,D& V’R(0#=’)*”D1″*-&’q’/&?(0)*”D1″*-&’”&,+01=(
CLINICAL PICTURE (Signs and symptoms)
Because many organs can be affected by myeloma, the symptoms and signs vary greatly. A mnemonic sometimes used to remember some of the common symptoms of multiple myeloma is CRAB: C = calcium (elevated), R = renal failure, A = anemia, B = bone lesions. Myeloma has many other possible symptoms, including opportunistic infections (e.g., pneumonia) and weight loss.
- Bone pain
Bone pain affects almost 70% of people with multiple myeloma and is the most common symptom. Myeloma bone pain usually involves the spine and ribs, and worsens with activity.
- Anemia
The anemia found in myeloma is usually normocytic and normochromic. It results from the replacement of normal bone marrow by infiltrating tumor cells and inhibition of normal red blood cell production (hematopoiesis) by cytokines.
- Impaired kidney function
Impaired kidney function may develop, either acutely or chronically, and with any degree of severity. The most common cause of kidney failure in multiple myeloma is due to proteins secreted by the malignant cells.
- Infection
The most common infections are pneumonias and pyelonephritis.
- Neurological symptoms
Some symptoms (e.g., weakness, confusion, and fatigue) may be due to anemia or hypercalcemia.
- Mouth symptoms may involve pain, numbness, swelling, expansion of the jaw etc
Diagnosis
The following tests are required for patients with suspected MM
- Serum protein electrophoresis (best initial test)
- Urine protein electrophoresis
- Bone marrow biopsy (confirmatory test)
- Laboratory tests (Complete blood Count and biochemistry) to assess for hypercalcemia, anemia and renal insufficiency
- Imaging to assess for bone lesions
109. Acromegaly. Gigantism. Dwarfism – etiology, pathogenesis, clinical presentation, diagnosis.
Acromegaly
Acromegaly is a hormonal disorder that develops when your pituitary gland produces too much growth hormone during adulthood. When this happens, your bones increase in size, including those of your hands, feet and face. Acromegaly usually affects middle-aged adults.
Etiology
Acromegaly is caused by the pituitary gland overproducing growth hormone (GH) over time. The pituitary gland, a small gland situated at the base of your brain behind the bridge of your nose, produces a number of hormones. GH plays an important role in managing your physical growth.
When GH is secreted into your bloodstream, it triggers your liver to produce a hormone called insulin-like growth factor-I (IGF-I). In turn, IGF-I stimulates the growth of bones and other tissues.
If your pituitary gland makes too much GH, excessive amounts of IGF-I can result. Too much IGF-I can cause abnormal growth of your soft tissues and skeleton and other signs and symptoms characteristic of acromegaly and gigantism.
In adults, a tumor is the most common cause of too much GH production:
- Pituitary tumors. Most cases of acromegaly are caused by a noncancerous (benign) tumor (adenoma) of the pituitary gland. The tumor secretes excessive amounts of growth hormone, causing many of the signs and symptoms of acromegaly. Some of the symptoms of acromegaly, such as headaches and impaired vision, are due to the tumor mass pressing on nearby brain tissues.
- Non Pituitary tumors. In a few people with acromegaly, tumors in other parts of the body, such as the lungs or pancreas, cause the disorder. Sometimes, these tumors secrete GH. In other cases, the tumors produce a hormone called growth hormone-releasing hormone (GH-RH), which stimulates the pituitary gland to make more GH.
Pathogenesis
- In pituitary adenomas, a mutation in the alpha subunit of the guanine nucleotide stimulatory protein is responsible for the excess growth hormone secretion.
- The mutation in the alpha subunit will lead to increased synthesis of cAMP which is responsible for the growth of certain cells.
- Increased synthesis of cAMP will result in the increased secretion of the growth hormone.
- Signal transduction and transcription (STAT) induce production of IGF-1 from liver, bone and pituitary gland.
- The IGF-1 is responsible for the acral features of acromegaly. IGF-1 causes the rapid increase in the hand and feet size, forehead protrusion, and jaw prominence.
- The high level of IGF-1 is responsible for the following pathologic processes:
- IGF-1 is responsible for the diabetes mellitus which is common in 20% of patients with acromegaly. IGF-1 interferes with insulin on its receptor which leads to insulin resistance and hyperglycemia.
- IGF-1 causes hypertrophy of the body organs like the heart (cardiomegaly) and tongue (macroglossia).
Clinical presentation
Acromegaly may produce the following signs and symptoms, which can vary from one person to another:
- Enlarged hands and feet
- Coarsened, enlarged facial features
- Coarse, oily, thickened skin
- Excessive sweating and body odor
- Small outgrowths of skin tissue (skin tags)
- Fatigue and muscle weakness
- A deepened, husky voice due to enlarged vocal cords and sinuses
- Severe snoring due to obstruction of the upper airway
- Impaired vision
- Headaches
- Enlarged tongue
- Pain and limited joint mobility
- Menstrual cycle irregularities in women
- Erectile dysfunction in men
- Enlarged organs, such as the heart
- Loss of interest in sex
Diagnosis
Your doctor will ask about your medical history and conduct a physical exam. Then he or she may recommend the following steps:
- GH and IGF-I measurement. After you’ve fasted overnight, your doctor will take a blood sample to measure your levels of GH and IGF-I. Elevated levels of these hormones suggest acromegaly.
- Growth hormone suppression test. This is the definitive method for verifying acromegaly. In this test, your blood levels of GH are measured before and after you drink a preparation of sugar (glucose). Normally, glucose ingestion depresses levels of GH. If you have acromegaly, your GH level will tend to stay high.
- Imaging. Your doctor may recommend that you undergo an imaging procedure, such as magnetic resonance imaging (MRI), to help pinpoint the location and size of a tumor of your pituitary gland. If no pituitary tumors are seen, your doctor may look for non pituitary tumors as the cause of your high GH levels.
Gigantism refers to abnormally high linear growth due to excessive action of insulin like growth factor I (IGF-I) while the epiphyseal growth plates are open during childhood. Acromegaly is the same disorder of IGF-I excess but occurs after the growth plate cartilage fuses in adulthood.
Gigantism
gigantism, is a condition characterized by excessive growth and height significantly above average. In humans, this condition is caused by overproduction of growth hormone in childhood resulting in people 7 to 9 ft (2.1 to 2.7 m) in height. it is a rare disorder resulting from increased levels of growth hormone before the fusion of the growth plate which usually occurs at some point soon after puberty. This increase is most often due to abnormal tumor growths on the pituitary gland. Gigantism should not be confused with acromegaly, the adult form of the disorder, characterized by somatic enlargement specifically in the extremities and face.[
Causes
Gigantism is characterized by an excess of growth hormone (GH). This overproduction of growth hormone that brings about gigantism is virtually always caused by pituitary growths (adenomas). These adenomas are on the anterior pituitary gland. They can also cause overproduction of GH’s hypothalamic precursor known as growth hormone releasing hormone (GHRH).
As a result of the excessive amounts of growth hormone, children achieve heights that are well above normal ranges.The specific age of onset for gigantism varies between patients and gender, but the common age that excessive growth symptoms start to appear has been found to be around 13 years. Other health complications, such as hypertension, may occur in pediatric patients with hyper-secretion of growth hormone. Characteristics more similar to those seen in acromegaly may occur in patients that are closer in age to adolescence since they are nearing growth plate fusion
Symptoms
- very large hands and feet
- thick toes and fingers
- a prominent jaw and forehead
- coarse facial features
Children with gigantism may also have flat noses and large heads, lips, or tongues.
The symptoms your child has may depend on the size of the pituitary gland tumor. As the tumor grows, it may press on nerves in the brain. Many people experience headaches, vision problems, or nausea from tumors in this area. Other symptoms of gigantism may include:
- excessive sweating
- severe or recurrent headaches
- weakness
- insomnia and other sleep disorders
- delayed puberty in both boys and girls
- irregular menstrual periods in girls
- deafness
Diagnosis
Blood test to measure levels of growth hormones and insulin-like growth factor 1 (IGF-1), which is a hormone produced by the liver. The doctor also may recommend an oral glucose tolerance test.
During an oral glucose tolerance test
In a normal body, growth hormone levels will drop after eating or drinking glucose. If your child’s levels remain the same, it means their body is producing too much growth hormone.
If the blood tests indicate gigantism, your child will need an MRI scan of the pituitary gland. Doctors use this scan to find the tumor and see its size and position.
Dwarfism
Dwarfism is short stature that results from a genetic or medical condition. Dwarfism is generally defined as an adult height of 4 feet 10 inches (147 centimeters) or less. The average adult height among people with dwarfism is 4 feet (122 cm). Many different medical conditions cause dwarfism.
Many different medical conditions cause dwarfism. In general, the disorders are divided into two broad categories:
- Disproportionate dwarfism. If body size is disproportionate, some parts of the body are small, and others are of average size or above-average size. Disorders causing disproportionate dwarfism inhibit the development of bones.
- Proportionate dwarfism. A body is proportionately small if all parts of the body are small to the same degree and appear to be proportioned like a body of average stature. Medical conditions present at birth or appearing in early childhood limit overall growth and development
Causes
Most dwarfism-related conditions are genetic disorders, but the causes of some disorders are unknown. Most occurrences of dwarfism result from a random genetic mutation in either the father’s sperm or the mother’s egg rather than from either parent’s complete genetic makeup.
Achondroplasia
About 80 percent of people with achondroplasia are born to parents of average height. A person with achondroplasia and with two average-size parents received one mutated copy of the gene associated with the disorder and one normal copy of the gene. A person with the disorder may pass along either a mutated or normal copy to his or her own children.
Turner syndrome
Turner syndrome, a condition that affects only girls and women, results when a sex chromosome (the X chromosome) is missing or partially missing. A female inherits an X chromosome from each parent. A girl with Turner syndrome has only one fully functioning copy of the female sex chromosome rather than two.
Growth hormone deficiency
The cause of growth hormone deficiency can sometimes be traced to a genetic mutation or injury, but for most people with the disorder, no cause can be identified.
Other causes
Other causes of dwarfism include other genetic disorders, deficiencies in other hormones or poor nutrition. Sometimes the cause is unknown.
Symptoms
- An average-size trunk
- Short arms and legs, with particularly short upper arms and upper legs
- Short fingers, often with a wide separation between the middle and ring fingers
- Limited mobility at the elbows
- A disproportionately large head, with a prominent forehead and a flattened bridge of the nose
- Progressive development of bowed legs
- Progressive development of swayed lower back
- An adult height around 4 feet (122 cm)
Diagnosis
Diagnostic tests may include:
- Measurements. A regular part of a well-baby medical exam is the measurement of height, weight and head circumference. At each visit, your pediatrician will plot these measurements on a chart to show your child’s current percentile ranking for each one. This is important for identifying abnormal growth, such as delayed growth or a disproportionately large head. If any trends in these charts are a concern, your pediatrician may make more-frequent measurements.
- Appearance. Many distinct facial and skeletal features are associated with each of several dwarfism disorders. Your child’s appearance also may help your pediatrician to make a diagnosis.
- Imaging technology. Your doctor may order imaging studies, such as Xrays, because certain abnormalities of the skull and skeleton can indicate which disorder your child may have. Various imaging devices may also reveal delayed maturation of bones, as is the case in growth hormone deficiency. A magnetic resonance imaging (MRI) scan may reveal abnormalities of the pituitary gland or hypothalamus, both of which play a role in hormone function.
- Genetic tests. Genetic tests are available for many of the known causal genes of dwarfism-related disorders, but these tests often aren’t necessary to make an accurate diagnosis. Your doctor is likely to suggest a test only to distinguish among possible diagnoses when other evidence is unclear or as a part of further family planning. If your pediatrician believes your daughter may have Turner syndrome, then a special lab test may be done that assesses the X chromosomes extracted from blood cells.
- Family history. Your pediatrician may take a history of stature in siblings, parents, grandparents or other relatives to help determine whether the average range of height in your family includes short stature.
- Hormone tests. Your doctor may order tests that assess levels of growth hormone or other hormones that are critical for childhood growth and development.
110. Diabetes insipidus – etiology, pathogenesis, clinical presentation, diagnosis.
Diabetes insipidus is an uncommon disorder that causes an imbalance of fluids in the body. This imbalance makes you very thirsty even if you’ve had something to drink. It also leads you to produce large amounts of urine. There’s no cure for diabetes insipidus. But treatments can relieve your thirst and decrease your urine output.
ETIOLOGY
- Central diabetes insipidus. Damage to the pituitary gland or hypothalamus from surgery, a tumor, a head injury or an illness can cause central diabetes insipidus by affecting the usual production, storage and release of ADH. An inherited genetic disease can also cause this condition.
- Nephrogenic diabetes insipidus. Nephrogenic diabetes insipidus occurs when there’s a defect in the kidney tubules — the structures in your kidneys that cause water to be excreted or reabsorbed. This defect makes your kidneys unable to properly respond to ADH.
The defect may be due to an inherited (genetic) disorder or a chronic kidney disorder. Certain drugs, such as lithium or antiviral medications such as foscarnet (Foscavir), also can cause nephrogenic diabetes insipidus.
- Gestational diabetes insipidus. Gestational diabetes insipidus is rare. It occurs only during pregnancy when an enzyme made by the placenta destroys ADH in the mother.
- Primary polydipsia. Also known as dipsogenic diabetes insipidus, this condition can cause production of large amounts of diluted urine. The underlying cause is drinking an excessive amount of fluids.
PATHOGENESIS
Diabetes insipidus occurs when your body can’t properly balance the body’s fluid levels. When your fluid regulation system is working properly, your kidneys help maintain this balance. The kidneys remove fluids from your bloodstream. This fluid waste is temporarily stored in your bladder as urine, until you urinate. The body can also rid itself of excess fluids through sweating, breathing or diarrhea. A hormone called anti-diuretic hormone (ADH), or vasopressin, helps control how fast or slow fluids are excreted. ADH is made in a part of the brain called the hypothalamus and stored in the pituitary gland, a small gland found in the base of the brain. If you have diabetes insipidus, your body can’t properly balance fluid levels.
CLINICAL PRESENTATION
- Extreme thirst
- Producing large amounts of diluted urine
- Frequent need to get up to urinate during the night
- Preference for cold drinks
If the condition is serious, urine output can be as much as 20 quarts (about 19 liters) a day if you’re drinking a lot of fluids. A healthy adult typically urinates an average of 1 or 2 quarts (about 1 to 2 liters) a day.
DIAGNOSIS
- medical and family history
- physical exam
- Urinalysis
- blood tests
- fluid deprivation test
- magnetic resonance imaging (MRI)
●
111. Thyrotoxicosis. Graves’ disease. Toxic adenoma-etiology, pathogenesis, clinical presentation, diagnosis.
THYROTOXICOSIS
Definition:
- Thyrotoxicosis is the state produced by excessive thyroid hormone.
- It is not strictly the same thing as hyperthyroidism, as thyrotoxicosis can exist without hyperthyroidism being present – for example – after the administration of excessive thyroxine that may be seen when hypothyroidism is treated.
- However, in clinical practice, the terms thyrotoxicosis and hyperthyroidism are often used interchangeably.
Epidemiology:
- Affects 2-5% of females and 0.2-03% of men, The female : male ratio is 5:1.
- Onset usually between ages of 20 and 40 in cases of Graves disease, but later in life where the cause is nodular thyroid disease.
- 99% of cases are caused by intrinsic thyroid disease, and less than 1% caused by a primary pituitary problem.
- Grave’s disease accounts for 60-80% of cases of thyrotoxicosis.
- Grave’s disease is an autoimmune disorder caused by the production of TSH receptor stimulating antibodies.
- These antibodies stimulate the thyroid gland to produce more T3 and T4 ● Nodular thyroid disease accounts for most of the rest (20-40%).
Etiology:
- Hyperfunctioning thyroid gland
- Destruction of the thyroid gland
- Exogenous hyperthyroidism
- Ectopic (extrathyroidal) hormone production Clinical presentation:
General symptoms:
- Hyperactivity, irritability, altered mood, excessive growth rate and height- esp in children
- Heat intolerance, sweating
- Palpitations, Fatigue, weakness. Weight loss with increased appetite
- Hyper-reflexia, Diarrhoea, steatorrhea, Polyuria, Loss of libido
- Oligomenorrhoea (infrequent periods), Menorrhagia (very heavy periods)
● Sinus tachycardia, Atrial fibrillation – particularly in elderly
- Fine tremor Warm, moist skin
- Goitre – in almost all cases (diffuse and symmetrical)
- Diffuse pigmentation, Palmar erythema
- Muscle weakness and wasting
● Eyelid retraction, Periorbital oedema, Proptosis – in 50% of graves cases
- Gynecomastia
- Thyrotoxic storm – severe acute presentation of thyrotoxicosis (thyrotoxic crisis). It has a 20-30% mortality rate. With this there is:
- A marked fever (>38.5’), Seizures, Vomiting, Diarrhoea, Jaundice
- Death – can be caused by arrhythmias, heart failure or hyperthermia
Diagnostics:
- Serum TSH will be low, around<0.05mU/L (norm. – 0.4-5 U/L) To confirm diagnosis – increased levels of T4 / T3 also needed
- TSH is usually the initial first test
- In all causes of thyrotoxicosis, TSH is suppressed and T3 and T4 are raised – Auto-antibodies:
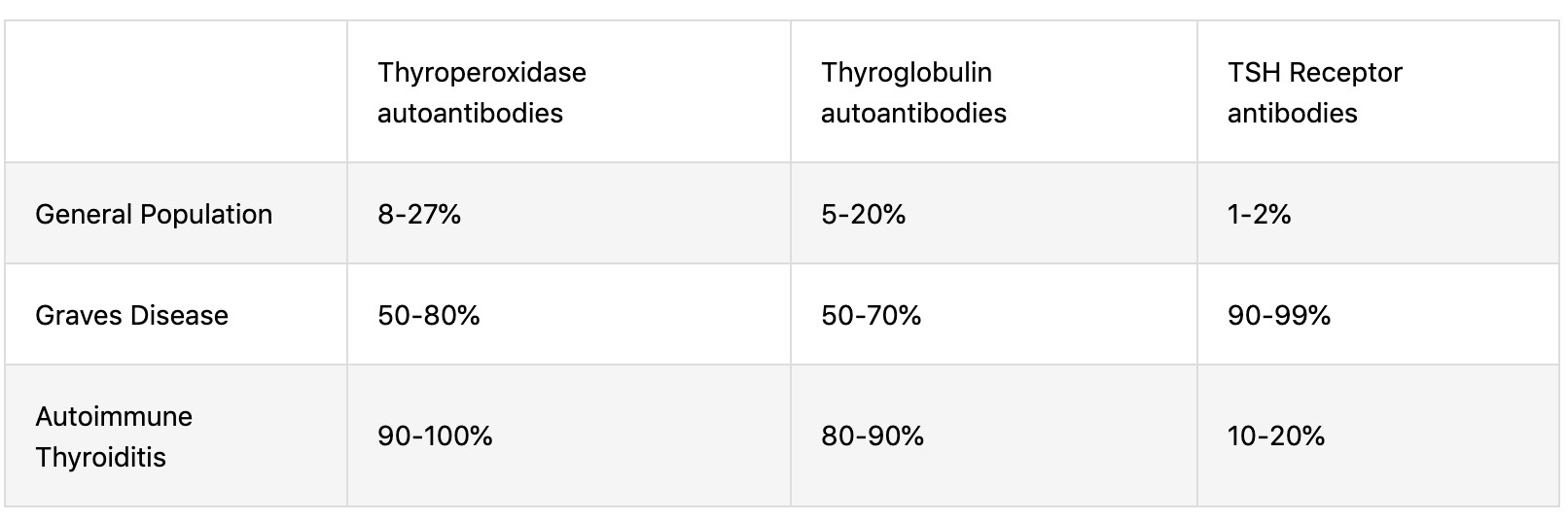 Imaging:
Imaging:
- Radionuclide scan is
the imaging modality of choice in differentiating
the cause of thyrotoxicosis – Results:
- Grave’s disease
– diffuse widespread uptake
- Toxic multinodular goitre – Can be normal, or may show multiple nodes of uptake, with the rest of the thyroid often showing reduced uptake
- Toxic adenoma – single area of increased uptake
- Thyroiditis – none or minimal uptake
- Ultrasound is often NOT useful in diagnosing the cause of thyrotoxicosis Treatment:
- Anti-thyroid drugs are the first line treatment for Grave’s disease. Radioactive iodine and thyroidectomy may also be considered. Symptomatic treatment and surgery is rare
GRAVES DISEASE
- Grave’s disease is an autoimmune disorder caused by the production of TSH receptor stimulating antibodies. Most common in women.
- These antibodies stimulate the thyroid gland to produce more T3 and T4 Etiology:
- Genetic predisposition – 50% of patients with Graves disease have a family history of autoimmune disorders (e.g., type 1 diabetes mellitus, Hashimoto disease, pernicious anemia, myasthenia gravis). Associated with HLA-DR3 and HLA-B8 alleles
- Autoimmunity: B and T lymphocyte-mediated disorder
- Triggers
- Infectious agents: Yersinia enterocolitica and Borrelia burgdorferi have been shown to trigger antigen mimicry for homologies between their protein constituents and thyroid autoantigens.
- Stress, Physical: surgery, trauma, Psychological, Pregnancy [2]
- Environmental factors: smoke, irradiations, drugs, endocrine disruptors Pathophysiology:
- General mechanism: B and T cell-mediated autoimmunity’q’?01+#D-*1,’1C’”-*=#%$-*,M’IgG against TSH-receptor (TRAb; type II hypersensitivity’0($D-*1,G’q’V’thyroid’C#,D-*1,’$,+’
M01.-/’q’hyperthyroidism and diffuse goiter
- Thyroid-associated ophthalmopathy: activated B and T cells infiltrate retro-orbital space targeting orbital fibroblasts’q’cytokine release (e.g. TNF-α, IFN-γG’q’%1D$%’*,C%$==$-10&’ 0(“?1,”(’q’fibroblast proliferation and differentiation to adipocytes’q’?01+#D-*1,’1C’ hyaluronic acid and GAGs and increased amount of adipocytes’q’*,D0($”(’*,’-/(’)1%#=(’1C’ *,-0$10>*-$%’C$-’$,+’=#”D%(’-*””#(“’q’exophthalmos, lid retraction, disturbances in ocular motility (causing diplopia)
- Pretibial myxedema: dermal fibroblast stimulation and deposition of glycosaminoglycans in connective tissue Clinical symptoms:
Symptoms of hyperthyroidism and Triad of Graves disease:
- Diffuse goiter: Smooth uniformly enlarged goiter, Bruit may be heard superior poles of the lobes
- Ophthalmopathy: Exophthalmos, Ocular motility disturbances, Lid retraction and conjunctival conditions
- Dermopathy (pretibial myxedema): non-pitting edema and firm plaques on the anterior/ lateral aspects of both legs Diagnosis:
– V’TRAbs’E”?(D*C*DG’’’’’’’’’’’’’’’’’’’’’’’’’’’9’V’Y,-*9fdt’$,+’$,-*9Tg (nonspecific)
- Thyroid scintigraphy : Indicated if TRAbs are low to establish a diagnosis (Contraindicated in pregnancy)
- Thyroid ultrasound (with color Doppler) – Indicated in pregnant women with low TRAbs. Shows an enlarged, hypervascular thyroid Treatment:
Beta blockers, antithyroid drugs etc
TOXIC ADENOMA
It is an autonomously functioning thyroid nodule that causes hyperthyroidism. Thyroid nodules are abnormal growths within the thyroid gland – present in 50% of the general population but only palpable in 5–10%. These nodules are almost always benign. Some autonomous nodules cause only subclinical hyperthyroidism, with suppressed thyroid-stimulating hormone (TSH) level and normal concentrations of free thyroid hormones.
Epidemiology
○ YDD1#,-“’C10’b’4‘KB5’1C’hyperthyroidism cases
○ ♀ > ♂, Seen mostly in patients 30–50 years of age
Pathophysiology
○ Gain-of-function mutations of TSH receptor gene’*,’$’”*,M%(’?0(D#0″10’D(%%’q’$#-1,1=1#”’ C#,D-*1,*,M’1C’-/(’thyroid follicular cells’1C’$’”*,M%(’,1+#%(’’q’C1D$%’hyperplasia of thyroid’ C1%%*D#%$0’D(%%”’q’toxic adenoma
○ The autonomous thyroid nodule overproduces thyroid hormones’q’hyperthyroidism’q’ +(D0($”(’*,’pituitary TSH’”(D0(-*1,’q’”#??0(“”*1,’1C’hormone production from the rest of the gland
Clinical features: hyperthyroidism
Diagnostics
- V’T3’$,+’W’TSH
- Thyroid scintigraphy: solitary, hot nodule
— Shows radioiodine uptake by the hyperfunctioning nodules with suppression of rest of the gland
Treatment
○ Control symptoms with beta-blockers and thioamides until euthyroidism is achieved
○ Definitive treatment: Radioactive iodine ablation or Lobectomy or hemithyroidectomy for pure toxic adenomas
112. Hypothyroidism. Endemic and sporadic goiter. Cretinism – etiology, pathogenesis, clinical presentation, diagnosis.
Hypothyroidism, also called underactive thyroid or low thyroid, is a disorder of the endocrine system in which the thyroid gland does not produce enough thyroid hormone.
Primary hypothyroidism
- Due to disease of the thyroid and TSH is increased ● Most common cause is autoimmune disease.
- Usually results from Hashimoto’s thyroiditis and is associated with firm Goiter or later with a shrunken fibrotic thyroid with little or no function.
- Second most common cause is post-therapeutic hypothyroidism especially after radioactive iodine therapy or surgery for hyperthyroidism or Goiter.
- Goitrous hypothyroidism may occur in endemic Goiter where iodine deficiency decreases thyroid hormone-genesis.
fRS’*”’0(%($”(+’qD$#”(“’-/(’-/&01*+’-1’(,%$0M(’$,+’-0$?’*1+*,(’$)*+%&’q’h1*-(0’ 0(“#%-“
- In patients taking lithium, hypothyroidism may occur and this may be due to lithium inhibiting hormone release by the thyroid.
Endemic Goiter is defined as thyroid enlargement that occurs in more than 10% of a population, and sporadic Goiter is a result of environmental or genetic factors that do not affect the general population.
Cretinismn
- Iodine deficiency can cause endemic cretinism in children; endemic cretinism is the most common cause of congenital hypothyroidism in severely iodine-deficient regions and a major cause of mental deficiency worldwide.
- Sporadic cretinism is the random occurrence of cretinism in non endemic areas. Due to non-functioning or absent thyroid glands
Secondary hypothyroidism:
- occurs when the hypothalamus produces insufficient thyrotropin-releasing hormone
(TRH) or the pituitary produces insufficient TSH
- deficient TSH secretion due to deficient TRH secretion is termed tertiary hypothyroidism.
CLINICAL PRESENTATION
- Classic symptoms of fatigue, dry-haired, thick-skinned, deep-voiced patients with weight gain, cold intolerance, bradycardia and constipation.
- Also with nonpitting edema (myxedema) and pitting edema of lower extremities
- Children with hypothyroidism may not show classic features but often have a slow growth velocity, poor school performance and sometimes arrest of pubertal development
DIAGNOSIS
Laboratory testing of thyroid stimulating hormone levels in the blood is considered the best initial test for hypothyroidism; a second TSH level is often obtained several weeks later for confirmation
- fRSq’=1″-’”(,”*-*)(’$,+’(%()$-(+’*,’?0*=$0&’/&?1-/&01*+*”=
- [0((’-/&01r*,(’Ef_G’q%1.’ ’
113. Hyperparathyroidism – etiology, pathogenesis, clinical presentation, diagnosis.
Hyperparathyroidism is where the parathyroid glands, which are in the neck near the thyroid gland, produce too much parathyroid hormone. This causes blood calcium levels to rise (hypercalcaemia). Left untreated, high levels of calcium in the blood can lead to a range of problems.
Etiology
The parathyroid glands maintain proper levels of both calcium and phosphorus in your body by turning the secretion of parathyroid hormone (PTH) off or on, much like a thermostat controls a heating system to maintain a constant air temperature. Vitamin D also is involved in regulating the amount of calcium in your blood.
Normally, this balancing act works well. When calcium levels in your blood fall too low, your parathyroid glands secrete enough PTH to restore the balance. PTH raises calcium levels by releasing calcium from your bones and increasing the amount of calcium absorbed from your small intestine.
When blood-calcium levels are too high, the parathyroid glands produce less PTH. But sometimes one or more of these glands produce too much hormone. This leads to abnormally high calcium levels and low phosphorus levels in your blood.
Calcium is best known for its role in keeping your teeth and bones healthy. But calcium also aids in the transmission of signals in nerve cells, and it’s involved in muscle contraction. Phosphorus, another mineral, works along with calcium in these areas.
Hyperparathyroidism may occur because of a problem with the parathyroid glands (primary hyperparathyroidism) or because of another disease that affects the glands’ function (secondary hyperparathyroidism).
Primary hyperparathyroidism
Primary hyperparathyroidism occurs because of some problem with one or more of the four parathyroid glands:
- A noncancerous growth (adenoma) on a gland is the most common cause.
- Enlargement (hyperplasia) of two or more parathyroid glands accounts for most other cases.
- A cancerous tumor is a very rare cause of primary hyperparathyroidism.
Primary hyperparathyroidism usually occurs randomly, but some people inherit a gene that causes the disorder.
Secondary hyperparathyroidism
Secondary hyperparathyroidism is the result of another condition that lowers calcium levels. This causes your parathyroid glands to overwork to compensate for the calcium loss. Factors that may contribute to secondary hyperparathyroidism include:
- Severe calcium deficiency. Your body may not get enough calcium from your diet, often because your digestive system doesn’t absorb the calcium from it.
- Severe vitamin D deficiency. Vitamin D helps maintain appropriate calcium levels in the blood. It also helps your digestive system absorb calcium from your food.
Your body produces vitamin D when your skin is exposed to sunlight. You also consume some vitamin D in food. If you don’t get enough vitamin D, then calcium levels may drop.
- Chronic kidney failure. Your kidneys convert vitamin D into a form that your body can use. If your kidneys work poorly, usable vitamin D may decline and calcium levels drop. Chronic kidney failure is the most common cause of secondary hyperparathyroidism.
●
Clinical presentation
Hyperparathyroidism is often diagnosed before signs or symptoms of the disorder are apparent. When symptoms do occur, they’re the result of damage or dysfunction in other organs or tissues due to high calcium levels in the blood and urine or too little calcium in bones.
Symptoms may be so mild and nonspecific that they don’t seem related to parathyroid function, or they may be severe. The range of signs and symptoms include:
- Osteoporosis
- Kidney stones
- Excessive urination
- Abdominal pain
- Tiring easily or weakness
- Depression or forgetfulness
- Bone and joint pain
- Frequent complaints of illness with no apparent cause
- Nausea, vomiting or loss of appetite
Diagnosis
Blood tests
If blood test results show you have high calcium levels in your blood, your doctor will likely repeat the test to confirm the results after you haven’t eaten for a period of time.
Many conditions can raise calcium levels. But your doctor can diagnose hyperparathyroidism if blood tests show you also have high levels of parathyroid hormone.
Additional diagnostic tests
After diagnosing hyperparathyroidism, your doctor will likely order more tests to rule out possible secondary causes, to identify possible complications and to judge the severity of the condition. These tests include:
- Bone mineral density test. This test is done to see if you have developed osteoporosis. The most common test to measure bone mineral density is dual energy X-ray absorptiometry (DEXA).
This test uses special X-ray devices to measure how many grams of calcium and other bone minerals are packed into a bone segment.
- Urine test. A 24-hour collection of urine can provide information on how well your kidneys work and how much calcium is excreted in your urine. This test may help in judging the severity of hyperparathyroidism or diagnosing a kidney disorder causing hyperparathyroidism. If a very low calcium level is found in the urine, this may mean it’s a condition that doesn’t need treatment.
- Imaging tests of kidneys. Your doctor may order an X-ray or other imaging tests of your abdomen to determine if you have kidney stones or other kidney abnormalities.
Imaging tests before surgery
If your doctor recommends surgery, he or she will likely use one of these imaging tests to locate the parathyroid gland or glands that are causing problems:
- Sestamibi parathyroid scan. Sestamibi is a radioactive compound that is absorbed by overactive parathyroid glands and can be detected by a scanner that detects radioactivity.
The normal thyroid gland also absorbs sestamibi. To eliminate uptake in the thyroid obscuring the uptake in a parathyroid adenoma, radioactive iodine, which is only taken up by the thyroid, also is given and the thyroid image is digitally subtracted.
Computerized tomography (CT) scanning may be combined with the sestamibi scan to improve detection of an abnormality.
- Ultrasound. Ultrasound uses sound waves to create images of your parathyroid glands and surrounding tissue.
A small device held against your skin (transducer) emits high-pitched sound waves and records the sound wave echoes as they reflect off internal structures. A computer converts the echoes into images on a monitor.
114. Hyperparathyroidism – etiology, pathogenesis, clinical presentation, diagnosis.
ETIOLOGY
Hyperparathyroidism is caused by factors that increase the production of parathyroid hormone.
The parathyroid glands maintain proper levels of both calcium and phosphorus in your body by turning the secretion of parathyroid hormone (PTH) off or on, much like a thermostat controls a heating system to maintain a constant air temperature. Vitamin D also is involved in regulating the amount of calcium in your blood. Normally, this balancing act works well. When calcium levels in your blood fall too low, your parathyroid glands secrete enough PTH to restore the balance. PTH raises calcium levels by releasing calcium from your bones and increasing the amount of calcium absorbed from your small intestine.
When blood-calcium levels are too high, the parathyroid glands produce less PTH. But sometimes one or more of these glands produce too much hormone. This leads to abnormally high calcium levels and low phosphorus levels in your blood. Calcium is best known for its role in keeping your teeth and bones healthy. But calcium also aids in the transmission of signals in nerve cells, and it’s involved in muscle contraction. Phosphorus, another mineral, works along with calcium in these areas. Hyperparathyroidism may occur because of a problem with the parathyroid glands (primary hyperparathyroidism) or because of another disease that affects the glands’ function (secondary hyperparathyroidism).
Primary hyperparathyroidism
Occurs because of some problem with one or more of the four parathyroid glands:
- A noncancerous growth (adenoma) on a gland is the most common cause.
- Enlargement (hyperplasia) of two or more parathyroid glands accounts for most other cases.
- A cancerous tumor is a very rare cause of primary hyperparathyroidism.
Primary hyperparathyroidism usually occurs randomly, but some people inherit a gene that causes the disorder.
Secondary hyperparathyroidism
Result of another condition that lowers calcium levels. This causes your parathyroid glands to overwork to compensate for the calcium loss. Factors that may contribute to secondary hyperparathyroidism include:
- Severe calcium deficiency. Your body may not get enough calcium from your diet, often because your digestive system doesn’t absorb the calcium from it.
- Severe vitamin D deficiency. Vitamin D helps maintain appropriate calcium levels in the blood. It also helps your digestive system absorb calcium from your food. Your body produces vitamin D when your skin is exposed to sunlight. You also consume some vitamin D in food. If you don’t get enough vitamin D, then calcium levels may drop.
- Chronic kidney failure. Your kidneys convert vitamin D into a form that your body can use. If your kidneys work poorly, usable vitamin D may decline and calcium levels drop. Chronic kidney failure is the most common cause of secondary hyperparathyroidism.
PATHOGENESIS
Hyperparathyroidism is when your parathyroid glands create too much parathyroid hormone in the bloodstream. These glands, located behind the thyroid at the bottom of your neck, are about the size of a grain of rice. The parathyroid glands produce parathyroid hormone. This hormone helps maintain an appropriate balance of calcium in the bloodstream and in tissues that depend on calcium for proper functioning.
CLINICAL PRESENTATION
Symptoms may be so mild and nonspecific that they don’t seem related to parathyroid function, or they may be severe. The range of signs and symptoms include:
- Osteoporosis
- Kidney stones
- Excessive urination
- Abdominal pain
- Tiring easily or weakness
- Depression or forgetfulness
- Bone and joint pain
- Frequent complaints of illness with no apparent cause ● Nausea, vomiting or loss of appetite
DIAGNOSIS
- Blood tests – Bone mineral density test
- Imaging tests of kidneys
– Urine test
115. Cushing disease and Cushing syndrome. Pheochromocytoma.
CUSHING’S SYNDROME
Etiology
- most common cause – iatrogenic, due to administration of glucocorticoids for therapeutic reasons.
- Endogenous Cushing’s syndrome – from production of excess cortisol (and other steroid hormones) by the adrenal cortex.
- Major cause – bilateral adrenal hyperplasia secondary to hypersecretion of adrenocorticotropic hormone (ACTH) by the pituitary (Cushing’s disease) or from ectopic sources such as small cell carcinoma of the lung; carcinoids of the bronchus, thymus, gut and ovary, medullary carcinoma of the thyroid; or pheochromocytoma.
- Adenomas or carcinomas of the adrenal gland account for 15–20% of endogenous Cushing’s syndrome cases. There is a female preponderance in endogenous Cushing’s syndrome except for the ectopic ACTH syndrome.
Clinical Features
- Common and nonspecific – central obesity, hypertension, osteoporosis, psychological disturbances, acne, hirsutism, amenorrhea, and diabetes mellitus.
- Specific – easy bruising, purple striae, proximal myopathy, fat deposition in the face and nuchal areas (moon facies and buffalo hump), and rarely androgenization. Thin, fragile skin, and plethoric moon facies also may be found.
- Hypokalemia and metabolic alkalosis are prominent, particularly with ectopic production of ACTH. Diagnosis
TREATMENT
- Transsphenoidal surgery for pituitary ACTH-secreting microadenomas is curative in 70– 80%, but long-term follow-up is required as tumors may recur.
- Radiation therapy used when a surgical cure is not achieved.
- Therapy of adrenal adenoma or carcinoma requires surgical excision; stress doses of glucocorticoids must be given pre- and postoperatively.
- Metastatic and unresectable adrenal carcinomas are treated with mitotane i
- On occasion, debulking of lung carcinoma or resection of carcinoid tumors can result in remission of ectopic Cushing’s syndrome.
- If the source of ACTH cannot be resected, medical management with ketoconazole (, metyrapone, or mitotane may relieve manifestations of cortisol excess.
- Some cases, bilateral total adrenalectomy is required to control hypercorticism.
- Pts with unresectable pituitary adenomas who have had bilateral adrenalectomy are at risk for Nelson’s syndrome (aggressive pituitary adenoma enlargement).
CUSHING’S DISEASE
- rare condition, more common in women and occurs between the ages of 20 and 50. ● A pituitary adenoma is the most common cause of Cushing disease.
- Adenoma (pituitary tumor) that is almost always benign – hard to diagnose as they’re small.
- Endocrinologists help with the diagnostic process
Symptoms
Changes in appearance:
- Wide, purple stretch marks on the skin (chest, armpits, abdomen, flanks)
- Rapid and unexplained weight gain with a rounder face and abdomen
- Increased fat in the neck and above the collarbone and upper back
- Skin changes (bruising without injury, acne, hair growth) and red cheeks Mood and thinking:
- Memory loss or not being able to think clearly, Depression, Mood and behavior disorders Others:
- Fatigue, Muscle weakness, Menstrual cycle disorders, Osteoporosis, High blood glucose
(diabetes), High blood pressure, Blood clots in leg veins, Heart attack, Stroke, Fracture Diagnosis
- difficult as symptoms can have many different causes and the elevated cortisol levels can happen in cycles. As a result, cortisol levels may not be elevated at the time of testing.
- Three tests are commonly used:
- Measures cortisol levels in the saliva between 11:00 p.m. and midnight. In healthy people, cortisol levels are very low during this period of time. In contrast, people with Cushing disease have high levels.
- Cortisol levels can also be measured in urine that has been collected over a 24hour period.
- People with suspected Cushing disease have cortisol levels measured the morning after taking a late-night dose of dexamethasone, a laboratory-made steroid. Normally, dexamethasone causes cortisol to drop to a very low level, but in people with Cushing disease, this doesn’t happen.
- If these tests show high cortisol levels, the doctor will then measure the ACTH level in the blood. In Cushing disease, the cortisol levels are high, and the ACTH levels are normal or high. If these results are seen, the doctor will schedule an MRI of the pituitary gland to pinpoint the location of any tumors.
TREATMENT
- The first choice – surgical removal of the tumor.
- Some may need to have repeat surgery.
- If not radiation therapy may treat any remaining tumor cells.
- Medications to block the adrenal glands from producing cortisol (such as ketoconazole, metyrapone or mitotane) can be used while waiting for radiation to have an effect. Dopamine agonist (cabergoline), Pasireotide – reduce ACTH levels and cortisol production.Mifepristone, a glucocorticoid agoinst, is another medication that stops cortisol from working on the body.
- Rarely, the adrenal glands are removed surgically to stop cortisol overproduction.
PHEOCHROMOCYTOMA
= are a type of tumor of the adrenal glands that can release high levels of epinephrine and norepinephrine.
Etiology
- Tumor arise from chromaffin cells, which are derived from the neural crest.
Localization
b’wB5’$+0(,$%’=(+#%%$’E?/&”*1%1M*D$%%&’$D-*)$-(+’>&’$D(-&%D/1%*,(G’ b’KB5’(r-0$9$+0(,$%’*,’-/(’”&=?$-/(-*D’M$,M%*$’ b’KB5’$-’=#%-*?%(’%1D$-*1,
- Doctors don’t know why most PCC tumors form.
- About 30% of cases seem to run in families. These are more likely to be cancerous than ones that appear at random.
- The majority are benign, unilateral, catecholamine-producing tumors.
- Rarely, pheochromocytomas also produce other hormones such as EPO.
- 25% of pheochromocytomas are hereditary. Associations include:
- Multiple endocrine neoplasia type 2 (MEN 2A, MEN 2B)
- Neurofibromatosis type 1 (NF1)
- Von Hippel-Lindau (VHL) disease
Symotms:
Some people with these tumors have high blood pressure all the time. For others, it goes up and down.
- Constipation
- Dizziness when standing
- Nausea
- Tremors
- Shortness of breath
- Pale skin
- Fast or uneven heartbeat (heart palpitations)
- Severe headache
- Stomach, side, or back pain
- Unusual sweating
- Vomiting
- Weight loss
- Weakness
- Anxiety attacks
These symptoms can come on suddenly, like an attack, several times a day. Or they can happen just a few times a month. As the tumor grows, the attacks may become stronger and may happen more often.
Attacks are set off by things like:
- Pressure on the tumor, Massage Medications, especially anesthesia or beta-blockers
- Emotional stress, Physical activity, Childbirth, Surgery, Foods with a lot of the amino acid tyramine, such as red wine, chocolate, or cheese
Diagnostics
- Laboratory tests
- Initial test: metanephrines (metabolites of catecholamines) in plasma (high sensitivity)
- Confirmatory test: metanephrines and catecholamines in 24-hour urine (high specificity)
- Clonidine suppression test (rarely used) – Principle of the test: In healthy patients, clonidine normally significantly decreases plasma catecholamine levels by at least 30%.
○ Evaluation of results: If pheochromocytoma is present, catecholamine levels will fail to decrease upon clonidine administration, as the tumor will continue to produce catecholamines.
- Genetic testing: if MEN2A, MEN2B, NF1, or VHL is suspected
Treatment
Operable disease:.
○ Preoperative blood pressure management: combined alpha and beta-adrenergic blockade
■ First, a non-selective alpha blocker is given : phenoxybenzamine blocks alpha-1 and alpha-2 adrenoceptors equally and irreversibly
■ After sufficient alpha-adrenergic blockade, a beta blocker may be started for additional blood pressure control and control of tachyarrhythmias.
○ Treatment of choice: laparoscopic tumor resection (adrenalectomy)
■ “No-touch” technique, Open surgical resection – reserved for large or invasive tumors.
Inoperable disease
○ Benign pheochromocytoma: primary therapy with phenoxybenzamine
○ Malignant pheochromocytoma: MIBG therapy ; otherwise, palliative treatment (chemotherapy, tumor embolization)
116. Addison’s Disease and acute adrenal insufficiency – etiology, pathogenesis, clinical picture.
Addison’s disease, also known as primary adrenal insufficiency and hypocortisolism, is a longterm endocrine disorder in which the adrenal glands do not produce enough steroid hormones .Adrenal insufficiency is a disorder that occurs when the adrenal glands don’t make enough of certain hormones. The adrenal glands are located just above the kidneys. Adrenal insufficiency can be primary, secondary, or tertiary. Primary adrenal insufficiency is often called Addison’s disease.
Adrenal insufficiency can affect your body’s ability to respond to stress and maintain other essential life functions. With treatment, most people with adrenal insufficiency can have a normal, active life.
Addison’s disease
Addison’s disease occurs when the adrenal glands are damaged and can’t make enough of the hormone cortisol and sometimes the hormone aldosterone.
Secondary adrenal insufficiency
Secondary adrenal insufficiency starts in the pituitary—a pea-sized gland at the base of the brain. The pituitary makes adrenocorticotropin (ACTH), a hormone that tells the adrenal glands to make cortisol. If the pituitary doesn’t make enough ACTH, the adrenal glands don’t make enough cortisol. Over time, the adrenal glands can shrink and stop working.
Tertiary adrenal insufficiency
Tertiary adrenal insufficiency starts in the hypothalamus, a small area of the brain near the pituitary. The hypothalamus makes corticotropin-releasing hormone (CRH), a hormone that tells the pituitary to make ACTH. When the hypothalamus doesn’t make enough CRH, the pituitary gland doesn’t make enough ACTH. In turn, the adrenal glands don’t make enough cortisol.
Onset of severe symptoms (adrenal crisis) may be precipitated by acute infection (a common cause, especially with septicemia).
Other causes include trauma, surgery, and Na loss from excessive sweating.
ETIOLOGY
In 70% of the cases, it is due to idiopathic atrophy of the adrenal cortex, probably caused by autoimmune processes. In the rest of cases, it results from destruction of the adrenal gland by granuloma (e.g., IB), tumour, amyloidosis, hemorrhage, or inflammatory necrosis.
Hypoadrenocorticism can also result from administration of drugs that block corticosteroid Synthesis. Addison’s disease may coexist with diabetes mellitus or hypothyroidism in polyglandular deficiency syndrome.
PATHOPHYSIOLOGY
Mineralocorticoid deficiency:
- Results in increased excretion of Na and decreased excretion of K in urine but also in sweat, saliva, and the GI tract. A low serum concentration of Na and a high concentration of K is the result.
- Causes severe dehydration, plasma hypertonicity, acidosis, decreased circulatory volume,
- hypotension, and, eventually, circulatory collapse.
- When adrenal insufficiency is caused by inadequate ACTH production, electrolyte levels are often normal.
Glucocorticoid deficiency:
- contributes to hypotension and causes severe insulin sensitivity and disturbances in carbohydrate, fat, and protein metabolism
- In the absence of cortisol, less carbohydrate is formed from protein leading to hypoglycemia and diminished glycogen.
- Weakness follows, due in part to deficient neuromuscular function ● Resistance to infection, trauma, and other stress is diminished.
- Myocardial weakness and dehydration reduce cardiac output, and circulatory failure can occur.
- Decreased blood cortisol results in increased pituitary ACTH production and increased blood B Lipotropin, which has melanocyte-stimulating activity and, together with ACTH, causes the hyperpigmentation of skin and mucous membranes characteristic of Addison’s disease
CLINICAL PICTURE
- Symptoms
- Weight loss
- Anorexia
- Malaise
- Weakness
- Fever
- Depression
- Impotence/amenorrhoea
- Nausea/vomiting; Diarrhoea
- Confusion
- Syncope from postural hypotension
- Abdominal pain
- Constipation
- Myalgia
- Joint or back pain
Signs
- Pigmentation, especially of new
- Scars and palmar creases
- Buccal pigmentation
- Postural hypotension
- Loss of weight
- General wasting
- Dehydration
- Loss of body hair (Vitiligo)
117. Diabetes mellitus – etiology, pathogenesis, biochemistry.
Diabetes is a metabolic disease, characterized by a disorder of carbohydrate, protein, and fat metabolism resulting from impaired release of insulin by the pancreatic beta cells, inadequate and defective insulin receptors or both.
Chronic hyperglycemia and other metabolic disorders of DM are associated with long term damage, dysfunction and failure of various organs such as retina, nerves, kidney and in addition an increased risk of cardiovascular diseases Diabetes.
Causes of type 1 diabetes
The exact cause of type 1 diabetes is unknown. What is known is that your immune system — which normally fights harmful bacteria or viruses — attacks and destroys your insulin-producing cells in the pancreas. This leaves you with little or no insulin. Instead of being transported into your cells, sugar builds up in your bloodstream (Autoimmune).
Causes of prediabetes and type 2 diabetes
In prediabetes — which can lead to type 2 diabetes — and in type 2 diabetes, your cells become resistant to the action of insulin, and your pancreas is unable to make enough insulin to overcome this resistance. Instead of moving into your cells where it’s needed for energy, sugar builds up in your bloodstream.
Exactly why this happens is uncertain, although it’s believed that genetic and environmental factors play a role in the development of type 2 diabetes too. Being overweight is strongly linked to the development of type 2 diabetes, but not everyone with type 2 is overweight.
Causes of gestational diabetes
During pregnancy, the placenta produces hormones to sustain your pregnancy. These hormones make your cells more resistant to insulin.
Normally, your pancreas responds by producing enough extra insulin to overcome this resistance. But sometimes your pancreas can’t keep up. When this happens, too little glucose gets into your cells and too much stays in your blood, resulting in gestational diabetes.
Risk factors for gestational diabetes
Any pregnant woman can develop gestational diabetes, but some women are at greater risk than are others. Risk factors for gestational diabetes include:
- Age. Women older than age 25 are at increased risk.
- Family or personal history. Your risk increases if you have prediabetes — a precursor to type 2 diabetes — or if a close family member, such as a parent or sibling, has type 2 diabetes. You’re also at greater risk if you had gestational diabetes during a previous pregnancy, if you delivered a very large baby or if you had an unexplained stillbirth.
- Weight. Being overweight before pregnancy increases your risk.
- Race. For reasons that aren’t clear, women who are black, Hispanic,
American Indian or Asian are more likely to develop gestational diabetes.
Pathogenesis and biochemistry
- Type 1 diabetes is an autoimmune disease in which islet destruction is caused primarily by immune effector cells reacting against endogenous β-cell antigens
- Type 1 diabetes can be subdivided into two types
- Type 1A immune-mediated diabetes
Type 1A diabetes is thought to be an autoimmune disorder resulting from a genetic predisposition
- Type 1B idiopathic (non–immune-related) diabetes.
Genetic susceptibility contributes to only a part of diabetes risk, and environmental factors must play a role. Viral infections have been suggested as triggers for development of the disease. Some studies suggest that viruses might share epitopes with islet antigens, and the immune response to the virus results in cross-reactivity and destruction of islet tissues, a phenomenon known as molecular mimicry.
– Type 1 diabetes is a catabolic disorder characterized by:
- Failure of self-tolerance in T cells specific for islet antigens causing TH1 cells (which may secrete cytokines, including IFN-γ and TNF, that injure β cells), and CD8+ CTLs (which kill β cells directly) to destroy the pancreas
- An absolute lack of insulin ( no secretion) an elevation in blood glucose
(hyperglycemia) and a breakdown of body fats and proteins
- The absolute lack of insulin in people with type 1 DM means that they are particularly prone to the development of ketoacidosis. One of the actions of insulin is the inhibition of lipolysis (i.e., fat breakdown) and release of free fatty acids (FFA) from fat cells. In the absence of insulin, ketosis develops when these fatty acids are released from fat cells and converted to ketones in the liver
- Because of the loss of insulin response, all people with type 1A diabetes require exogenous insulin replacement to reverse the catabolic state, control blood glucose levels, and prevent ketosis.
Pathogenesis of Type 2 Diabetes Mellitus
Type 2 diabetes is a complex disease that involves an interplay of genetic and environmental factors and a proinflammatory state.
The metabolic abnormalities that lead to type 2 diabetes include:
1. Insulin resistance
- Insulin resistance is the failure of target tissues to respond normally to insulin.
- The liver, skeletal muscle and adipose tissue are the major tissues where insulin resistance manifests in abnormal glucose tolerance.
- Insulin resistance results in:
- Failure to inhibit endogenous glucose production (gluconeogenesis) in the liver, which contributes to high fasting blood glucose levels
- Failure of glucose uptake and glycogen synthesis to occur in skeletal muscle following a meal, which contributes to high post-prandial blood glucose level
- Failure to inhibit lipoprotein lipase in adipose tissue, leading to excess circulating free fatty acids (FFAs), which in turn, amplify the state of insulin resistance by blocking insulin receptors
- Functional defects in the insulin signaling pathway in states of insulin resistance.
- For example, reduced levels of the glucose transporter GLUT-4 on the cell surface
- In fact, one of the mechanisms by which exercise can improve insulin sensitivity is through increased translocation of GLUT-4 to the surface of skeletal muscle cells.
118. Diabetes mellitus – clinical picture, complications, diagnosis.
Diabetes mellitus refers to a group of diseases that affect how your body uses blood sugar (glucose). Glucose is vital to your health because it’s an important source of energy for the cells that make up your muscles and tissues. It’s also your brain’s main source of fuel. The underlying cause of diabetes varies by type. But, no matter what type of diabetes you have, it can lead to excess sugar in your blood. Too much sugar in your blood can lead to serious health problems.
Chronic diabetes conditions include type 1 diabetes and type 2 diabetes. Potentially reversible diabetes conditions include prediabetes — when your blood sugar levels are higher than normal, but not high enough to be classified as diabetes — and gestational diabetes, which occurs during pregnancy but may resolve after the baby is delivered.
TYPE 1
The exact cause of type 1 diabetes is unknown. What is known is that your immune system — which normally fights harmful bacteria or viruses — attacks and destroys your insulin-producing cells in the pancreas. This leaves you with little or no insulin. Instead of being transported into your cells, sugar builds up in your bloodstream. Type 1 is thought to be caused by a combination of genetic susceptibility and environmental factors, though exactly what those factors are is still unclear. Weight is not believed to be a factor in type 1 diabetes.
TYPE 2
In prediabetes — which can lead to type 2 diabetes — and in type 2 diabetes, your cells become resistant to the action of insulin, and your pancreas is unable to make enough insulin to overcome this resistance. Instead of moving into your cells where it’s needed for energy, sugar builds up in your bloodstream. Exactly why this happens is uncertain, although it’s believed that genetic and environmental factors play a role in the development of type 2 diabetes too. Being overweight is strongly linked to the development of type 2 diabetes, but not everyone with type 2 is overweight.
CLINICAL PRESENTATION
- Increased thirst
- Frequent urination
- Extreme hunger
- Unexplained weight loss
- Presence of ketones in the urine (ketones are a byproduct of the breakdown of muscle and fat that happens when there’s not enough available insulin)
- Fatigue
- Irritability
- Blurred vision
- Slow-healing sores
- Frequent infections, such as gums or skin infections and vaginal infections
Type 1 diabetes can develop at any age, though it often appears during childhood or adolescence. Type 2 diabetes, the more common type, can develop at any age, though it’s more common in people older than 40.
COMPLICATIONS
- Cardiovascular disease. Diabetes dramatically increases the risk of various cardiovascular problems, including coronary artery disease with chest pain (angina), heart attack, stroke and narrowing of arteries (atherosclerosis). If you have diabetes, you’re more likely to have heart disease or stroke.
- Nerve damage (neuropathy). Excess sugar can injure the walls of the tiny blood vessels (capillaries) that nourish your nerves, especially in your legs. This can cause tingling, numbness, burning or pain that usually begins at the tips of the toes or fingers and gradually spreads upward.
- Kidney damage (nephropathy). The kidneys contain millions of tiny blood vessel clusters (glomeruli) that filter waste from your blood. Diabetes can damage this delicate filtering system. Severe damage can lead to kidney failure or irreversible end-stage kidney disease, which may require dialysis or a kidney transplant.
- Eye damage (retinopathy). Diabetes can damage the blood vessels of the retina (diabetic retinopathy), potentially leading to blindness. Diabetes also increases the risk of other serious vision conditions, such as cataracts and glaucoma.
- Foot damage. Nerve damage in the feet or poor blood flow to the feet increases the risk of various foot complications. Left untreated, cuts and blisters can develop serious infections, which often heal poorly. These infections may ultimately require toe, foot or leg amputation.
- Skin conditions. Diabetes may leave you more susceptible to skin problems, including bacterial and fungal infections.
- Hearing impairment. Hearing problems are more common in people with diabetes.
- Alzheimer’s disease. Type 2 diabetes may increase the risk of dementia, such as Alzheimer’s disease. The poorer your blood sugar control, the greater the risk appears to be. Although there are theories as to how these disorders might be connected, none has yet been proved.
- Depression. Depression symptoms are common in people with type 1 and type 2 diabetes. Depression can affect diabetes management.
DIAGNOSIS
- Glycated hemoglobin (A1C) test
- Random blood sugar test
- Fasting blood sugar test
- Oral glucose tolerance test
- Gout – etiology, pathogenesis, clinical presentation, diagnosis.
Gout is a metabolic disease that most often affects middle-aged to elderly men and postmenopausal women. It results from an increased body pool of urate with hyperuricemia. Characterized by episodic acute arthritis or chronic arthritis caused by deposition of MSU crystals in joints and connective tissue tophi and the risk for deposition in kidney interstitium or uric acid nephrolithiasis.
ACUTE AND CHRONIC ARTHRITIS
- Acute arthritis is the most common early clinical manifestation of gout.
- Only one joint is affected initially, but polyarticular acute gout can occur in subsequent episodes.
- The metatarsophalangeal joint of the first toe often is involved, but tarsal joints, ankles, and knees also are affected commonly.
- Especially in elderly patients or in advanced disease, finger joints may be involved.
- Inflamed Heberden’s or Bouchard’s nodes may be a first manifestation of gouty arthritis.
- The first episode of acute gouty arthritis frequently begins at night with dramatic joint pain and swelling.
- Joints rapidly become warm, red, and tender, with a clinical appearance that often mimics that of cellulitis.
- Early attacks subsides spontaneously within 3–10 days, and most have intervals of varying length with no residual symptoms until the next episode.
- Several events may precipitate acute gouty arthritis: dietary excess, trauma, surgery, excessive ethanol ingestion, hypouricemic therapy, and serious medical illnesses such as myocardial infarction and stroke.
- After many acute mono- or oligoarticular attacks, a proportion of gouty patients may present with a chronic non symmetrical synovitis, causing confusion with rheumatoid arthritis.
- Less commonly, chronic gouty arthritis will be the only manifestation, and, more rarely, the disease will manifest only as periarticular tophaceous deposits in the absence of synovitis.
- Women represent only 5–20% of all patients with gout. Most women with gouty arthritis are postmenopausal and elderly, have osteoarthritis and arterial hypertension that causes mild renal insufficiency, and usually are receiving diuretics. Premenopausal gout is rare. Kindreds of precocious gout in young women caused by decreased renal urate clearance and renal insufficiency have been described.
Laboratory Diagnosis
- by needle aspiration of acutely or chronically involved joints or tophaceous deposits.
 During acute gouty attacks, needle-shaped MSU crystals typically are seen both intracellularly and extracellularly.
During acute gouty attacks, needle-shaped MSU crystals typically are seen both intracellularly and extracellularly.- Synovial fluid leukocyte counts are elevated from 2000 to 60,000/µL.
- Effusions appear cloudy due to the increased numbers of leukocytes.
- Large amounts of crystals occasionally produce a
thick pasty or chalky joint fluid. Bacterial infection can coexist with urate crystals in synovial fluid; if there is any suspicion of septic arthritis, joint fluid must be cultured.
- MSU crystals also demonstrated in the first metatarsophalangeal joint and in knees not acutely involved with gout. Arthrocentesis of these joints is a useful technique to establish the diagnosis of gout between attacks.
- Serum uric acid levels can be normal or low at the time of an acute attack, as inflammatory cytokines can be uricosuric and effective initiation of hypouricemic therapy can precipitate attacks. This limits the value of serum uric acid determinations for the diagnosis of gout.
- Serum urate levels are elevated at some time and are important to use to follow the course of hypouricemic therapy. A 24-h urine collection for uric acid can, in some cases, be useful in assessing the risk of stones, elucidating overproduction or underexcretion of uric acid, and deciding whether it may be appropriate to use a uricosuric therapy.
- Excretion of >800 mg of uric acid per 24 h on a regular diet suggests that causes of overproduction of purine should be considered.
- Urinalysis, serum creatinine, hemoglobin, white blood cell (WBC) count, liver function tests, and serum lipids should be obtained because of possible pathologic sequelae of gout and other associated diseases requiring treatment and as baselines because of possible adverse effects of gout treatment.
Radiographic Features
- Cystic changes, well-defined erosions with sclerotic margins (often with overhanging bony edges), and soft tissue masses are characteristic radiographic features of advanced chronic tophaceous gout.
- Ultrasound – aid earlier diagnosis, shows double contour sign overlying the articular cartilage.
- Dual-energy computed tomography (CT) – show specific features of presence of urate
crystals.
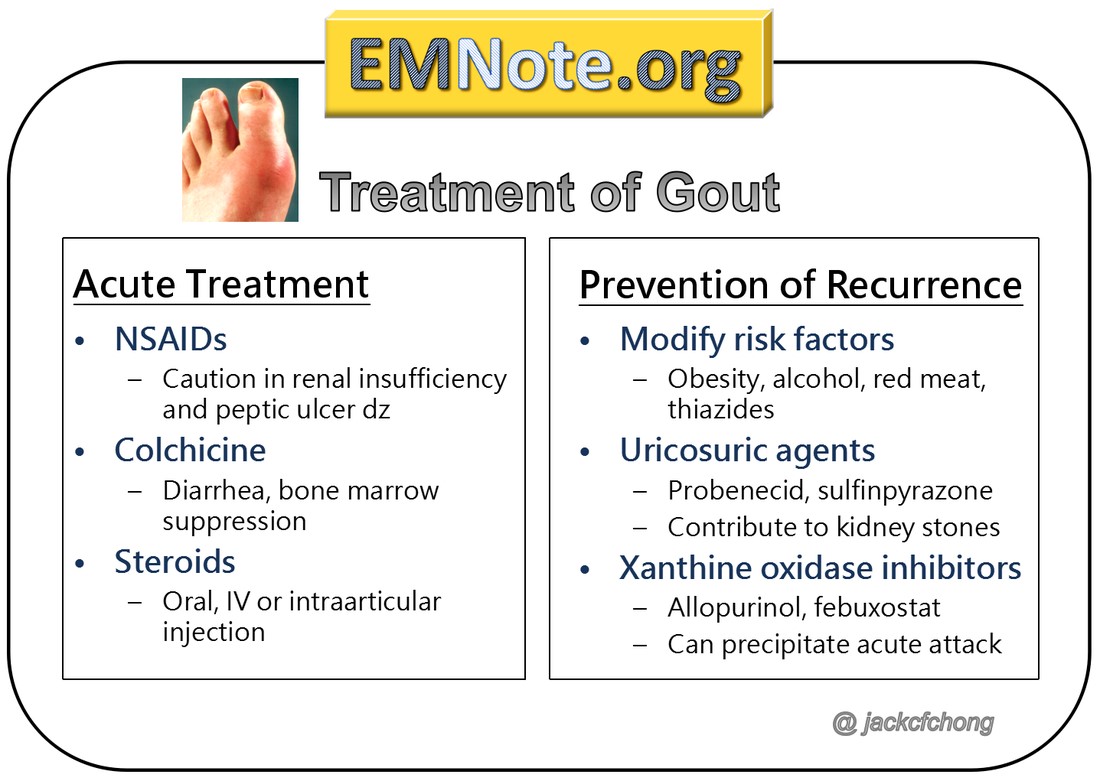
- Rheumatoid arthritis – etiology, pathogenesis, clinical presentation, diagnosis.
Rheumatoid arthritis (RA) is an inflammatory autoimmune disorder characterized by joint pain, swelling, and synovial destruction. RA predominantly affects middle-aged women. The condition can also cause various extra-articular manifestations such as rheumatoid nodules and pulmonary fibrosis.
Etiology
- Chronic inflammatory autoimmune disorder of unknown etiology
Hypotheses suggest the etiology is multifactorial, with the following factors playing a role:
- Genetic disposition: RA appears to be associated with specific HLA types (HLA-DR4, HLA-DR1).
- Environmental triggers (e.g., infection, tobacco)
- Hormonal factors Pathophysiology
- Initially, non-specific inflammation affects the synovial tissue, which is later amplified by activation of T cells (autoimmune response).
- With time, it may lead to inflammatory joint effusion and synovial hypertrophy, as well as progressive destruction and deterioration of cartilage and bone.
○ Synovial lining hyperplasia
○ d$,,#”’C10=$-*1,’$%1,M’-/(’”&,1)*$%’-*””#(’q’?01+#D(’?01-($”(“’q’+(“-01&’ D$0-*%$M(’(r-0$D(%%#%$0’=$-0*r
- Patients with positive rheumatoid factor (RF) are more likely to develop extra-articular manifestations of rheumatoid arthritis.
Clinical features
Articular manifestations
- Polyarthralgia
- Symmetrical pain and swelling of affected joints (also at rest).
- Frequently affected joints
- Metacarpophalangeal joints (MCPJs)
○ Proximal interphalangeal joints (PIPJs)
○ Wrist joints
○ Knee joints
Joints of the axial skeleton are usually spared except for the cervical spine (see RA of the cervical spine)
- Morning stiffness > 30 min; often improves with activity
- Joint deformities
- “Rheumatoid hand” is characteristic, and can include the following deformities:
○ Deepening of the interosseous spaces of the dorsum of hand ○ Swan neck deformity: PIP hyperextension and DIP flexion
○ Boutonniere deformity: PIP flexion and DIP hyperextension.
○ Hitchhiker thumb deformity (Z deformity of the thumb): hyperextension of the interphalangeal joint with fixed flexion of the MCP joint
○ Ulnar deviation of the fingers
- Hammer toe
- Atlanto-axial subluxation
Extra-articular manifestations
- Constitutional symptoms: low-grade fever, myalgia, malaise, night sweats
- Skin: rheumatoid nodules (common); non-tender, firm, subcutaneous swellings (2 mm–5 cm)
- Lungs: fibrosis, nodules, pleuritis, and pleural effusions
- Eye: keratoconjunctivitis sicca, scleritis, and episcleritis
- Endocrine and exocrine glands: secondary Sjögren syndrome
- Hematological: anemia of chronic disease
- Other musculoskeletal
○ Tenosynovitis and bursitis
○ Carpal tunnel syndrome (entrapment neuropathy)
■ Typical nocturnal paresthesia of volar hand and fingers I–III
■ Y-01?/&’1C’-/(,$0’=#”D%(“’q’+*CC*D#%-&’=$8*,M’$’C*”-z’*,$>*%*-&’-1’1??1″(’-/(’ -/#=>
- Tarsal tunnel syndrome
- Heart: pericarditis and myocarditis; higher risk of myocardial infarction, stroke, and CHF
- Vascular: peripheral vasculitis manifesting as livedo reticularis, Raynaud phenomenon, purpura, necrosing fingertips or peripheral neuropathy
Diagnosis is mainly based on clinical features (e.g., morning stiffness, symmetrical joint swelling) and laboratory tests (e.g., anti-CCP). X-ray findings (e.g., soft tissue swelling or joint space narrowing) occur late in the disease and are therefore not typically used for diagnosis.
Synovial fluid analysis
● Synovial fluid is collected by joint aspiration.
Findings
○ Cloudy yellow appearance
○ Sterile specimen with leukocytosis (WBC: 5,000–50,000/µL)
○ V’@(#-01?/*%”6’M0$,#%1D&-(“6’$,+’0$M1D&-(“’
○ V’d01-(*,”6’W’)*”D1″*-&
○ Possibly rheumatoid factor
Early intervention with disease-modifying antirheumatic drugs (DMARDs) plays a decisive role in successful treatment. RA is not curable, but early effective treatment may help offset severe complications (e.g., permanent damage to the affected joints).
121. Ankylosing spondylitis (Bechterew disease) – etiology, pathogenesis, clinical presentation, diagnosis.
Ankylosing spondylitis is an inflammatory disease that, over time, can cause some of the small bones in your spine (vertebrae) to fuse. This fusing makes the spine less flexible and can result in a hunched-forward posture. Etiology
Unknown but there seems to be a link to the HLA-B27 gene.
HLA-B27 gene
Research has shown more than 9 out of 10 people with AS carry a particular gene known as human leukocyte antigen B27 (HLA-B27).
Having this gene does not necessarily mean you’ll develop AS. It’s estimated 8 in every
100 people in the general population have the HLA-B27 gene, but most do not have AS.
It’s thought having this gene may make you more vulnerable to developing AS. The condition may be triggered by 1 or more environmental factors, although it’s not known what these are.
Pathogenesis
Recent genetic and immunological research has highlighted a key role for IL-17 A/IL-23 cytokine dysregulation in the aetiology of AS. Together with genetic data and the results of clinical trials of IL-17 A–neutralizing antibodies, this strongly supports the concept of SpA as a type 17-driven inflammatory disease.
HLA-B27 and AS
Despite intensive research, the pathogenic role of HLA-B27 remains unclear. Three major theories explaining the role of HLA-B27 in disease—the arthritogenic peptide theory, the misfolded HLA-B27 hypothesis and the cell-surface homodimers hypothesis
—have been put forward with varying degrees of evidence
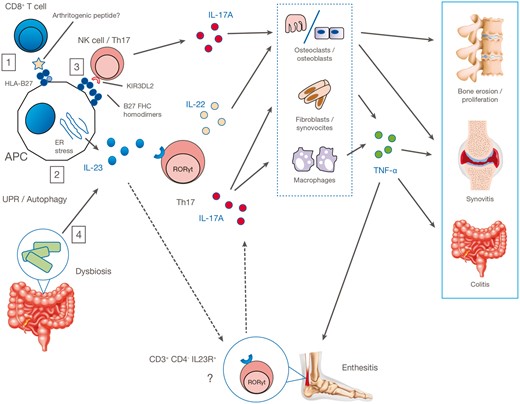
Clinical presentation
In the early stages, ankylosing spondylitis is likely to cause::
- stiffness and pain in your lower back in the early morning that lasts at least 30 minutes and then eases through the day or with activity
- pain that wakes you in the night
- pain in one or both buttocks and sometimes the backs of the thighs.
The condition can sometimes be mistaken for common backache.
Common backache often comes in short and painful spells. But the pain from ankylosing spondylitis is likely to be long lasting.
You may also have neck, shoulder, hip or thigh pain, which is worse when you’ve not been active for a time, for example if you sit for long periods working at a desk. Some people have pain, stiffness and swelling in their knees or ankles.
The pain and stiffness can vary over time. If most of the spine is affected, it can cause difficulty with activities that involve bending, twisting or turning.
Other possible symptoms include:
- soreness at the heel or in the arch of your foot
- pain and swelling in a finger or toe
- tenderness at the base of your pelvis, which can make sitting on a hard chair uncomfortable
- chest pain or a tightness around the chest that comes on gradually. This can make it difficult to take deep breaths. Your ribs may feel very tender, and you may find that you’re short of breath after even gentle activity. Coughing or sneezing may cause discomfort or pain.
- inflammation of the bowel. People with ankylosing spondylitis can develop bowel problems known as inflammatory bowel disease (IBD) or colitis. It’s a good idea to see your doctor if you have diarrhoea for more than two weeks or have bloody or slimy stool.
- fatigue, which is severe tiredness that doesn’t improve with sleep or rest. This can be caused by the condition itself, as well as by anaemia. This is when people have a lack of red blood cells, which carry oxygen around the body.
- depression and anxiety.
- inflammation of the eye, called either uveitis or iritis. The first signs are usually a painful and sometimes red eye. It may become uncomfortable to look at bright lights.
If one or both of your eyes are painful or red, or if you have changes to your vision such as partial loss of sight, blurred vision, floaters or sensitivity to light, it’s very important to get medical help as soon as possible.
Diagnosis
There is no one test that can show for certain that you have ankylosing spondylitis. A diagnosis will be made based on several things, including:
- the history of your condition and the symptoms you’ve experienced, including whether pain and discomfort is waking you up during the second half of the night
- a physical examination
- blood tests, which may show inflammation
- x-rays or a magnetic resonance imaging (MRI) scan
- your age. It can be diagnosed at any age, but most often begins before the age of 40, and often much younger.
122. Osteoarthritis – etiology, pathogenesis, clinical presentation, diagnosis.
Osteoarthritis (OA) causes inflammation in the joints and the breakdown and gradual loss of joint cartilage. As the cartilage wears down, a person experiences pain and difficulty with movement.
ETIOLOGY
| ● | joint injury – overusing your joint when it has not had enough time to heal after an injury or operation |
| ● | other conditions (secondary arthritis) – osteoarthritis can happen in joints severely damaged by a previous or existing condition, such as rheumatoid arthritis or gout |
| ● | age – your risk of developing the condition increases as you get older. |
| ● | family history – osteoarthritis may run in families, although studies have not identified a single gene responsible |
| ● | obesity – being obese puts excess strain on your joints, particularly those that bear most of your weight, such as your knees and hips |
| ● | being a woman – osteoarthristis is more common in women than men. |
PATHOGENESIS
Osteoarthritis occurs when the cartilage that cushions the ends of bones in your joints gradually deteriorates. Cartilage is a firm, slippery tissue that enables nearly frictionless joint motion. Eventually, if the cartilage wears down completely, bone will rub on bone. Osteoarthritis has often been referred to as a “wear and tear” disease. But besides the breakdown of cartilage, osteoarthritis affects the entire joint. It causes changes in the bone and deterioration of the connective tissues that hold the joint together and attach muscle to bone. It also causes inflammation of the joint lining.
CLINICAL PRESENTATION
- pain and stiffness that worsen after not moving the joint for a while
- swelling
- difficulty moving the affected joint
- warmth and tenderness in the joints
- a loss of muscle bulk
- a grating or crackling sound in the joint, known as crepitus
DIAGNOSIS
- X-rays
- MRI
- Blood tests
- Joint fluid analysis